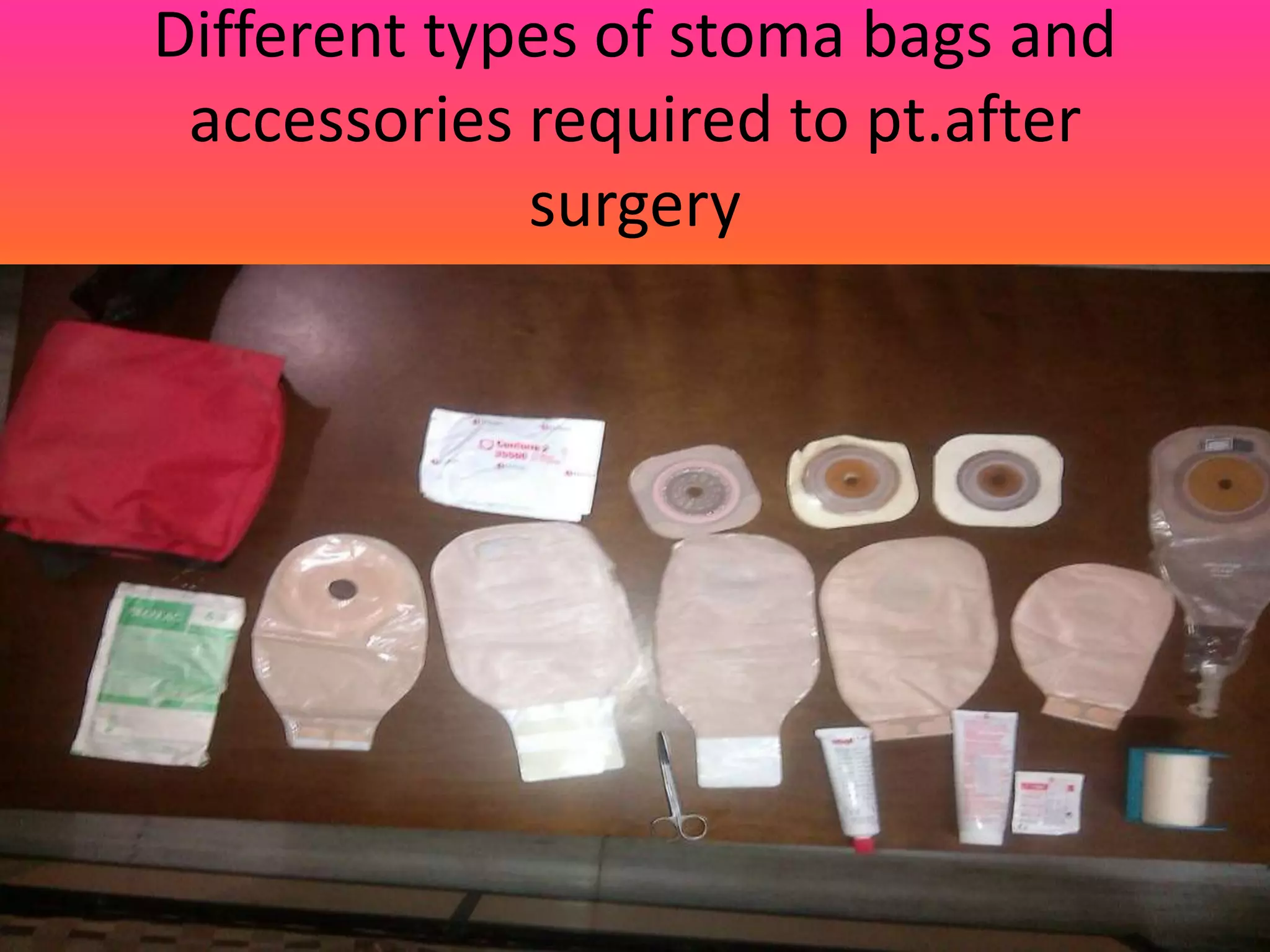
The document discusses the most common problems arising from ileostomy, including psychological issues, leakage, skin excoriation, and nutritional deficiencies. It emphasizes the importance of stoma care management for patients and their families, including education on pouching techniques, dietary restrictions, and addressing complications like food blockage. Additionally, it highlights the need for ongoing support and adjustment to lifestyle changes post-surgery.