1) Mastectomy is the surgical removal of breast tissue, either partially or completely. It is commonly performed to treat breast cancer.
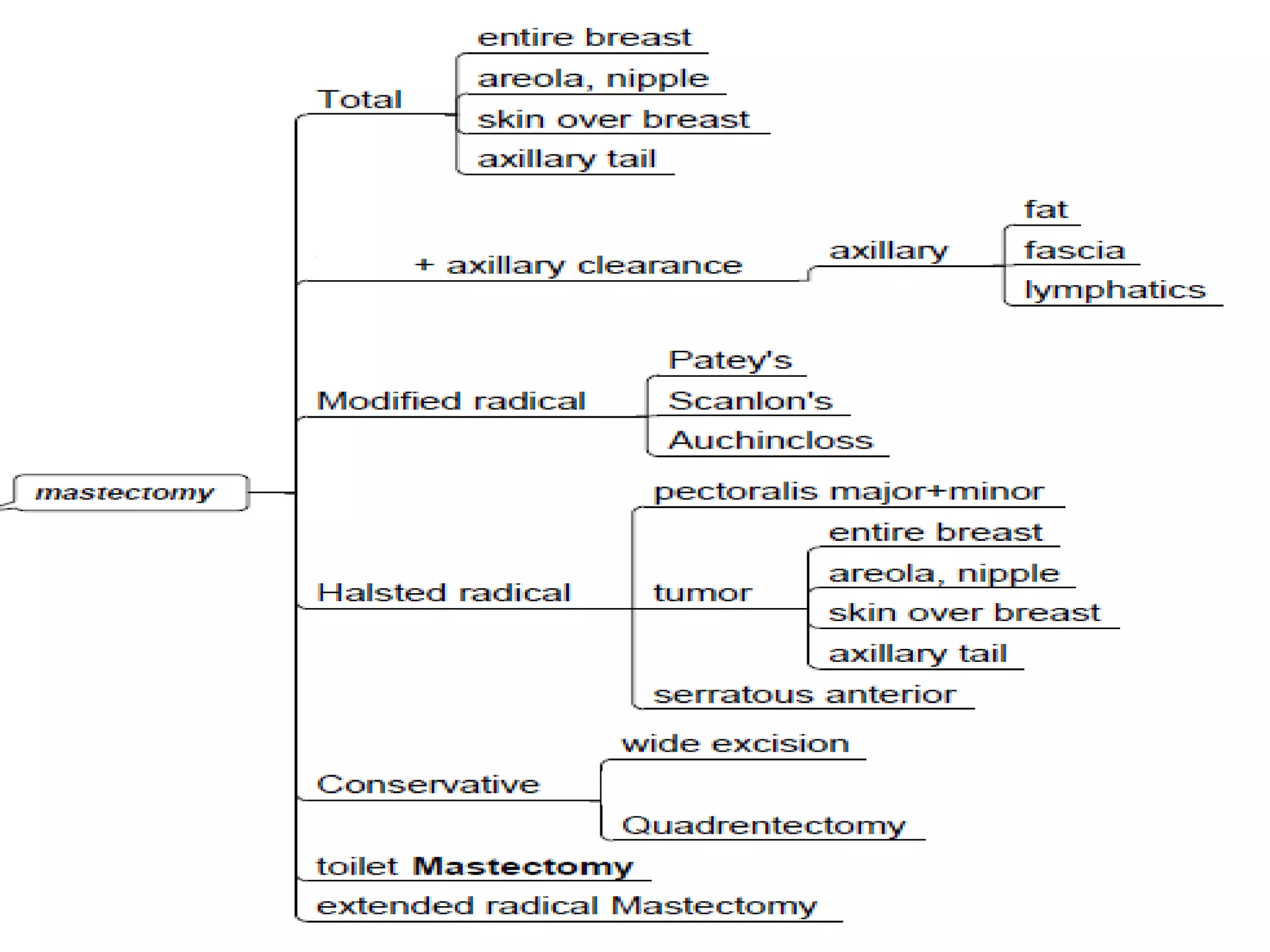
2) There are several types of mastectomy procedures including simple/total mastectomy, modified radical mastectomy, and breast conserving surgery.
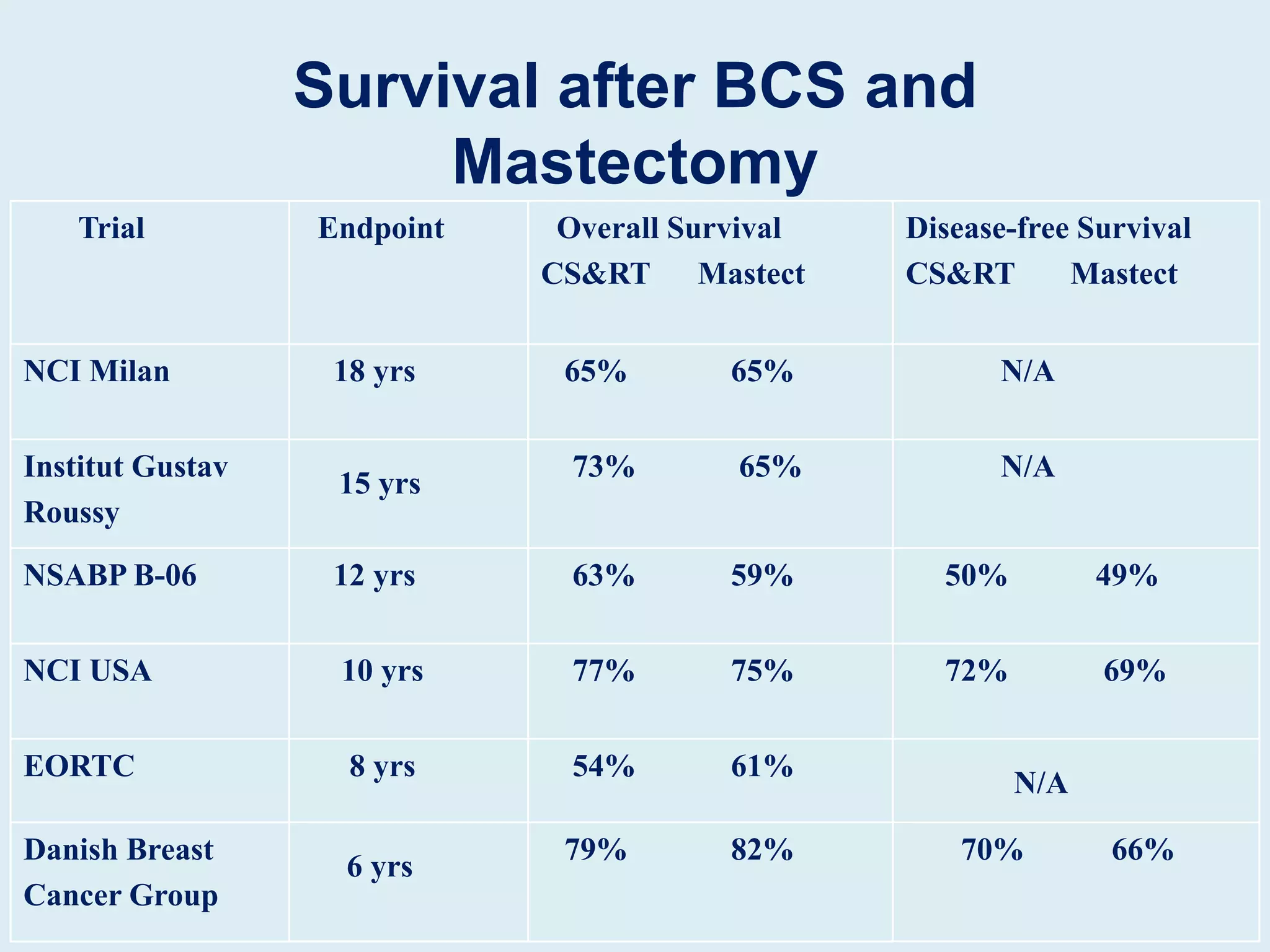
3) Factors such as tumor size, lymph node involvement, and patient preferences help determine which mastectomy procedure is most suitable. Post-operative care and follow up is also important after mastectomy.