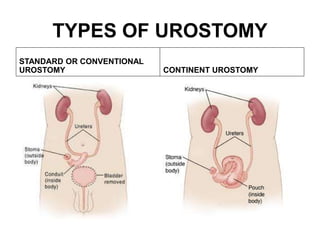
An ostomy is a surgically created opening in the small or large intestine to divert fecal matter. It is indicated for various intestinal diseases and injuries. There are three main types - colostomy, ileostomy, and urostomy - which are located and have characteristics depending on the portion of intestine used. Proper ostomy care involves assessing the stoma, applying pouches and barriers to protect the skin, managing diet and output, and educating patients.
















































































































![epidemiology.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/epidemiology-221129052007-92b54bb8-thumbnail.jpg?width=640&height=640&fit=bounds)



















