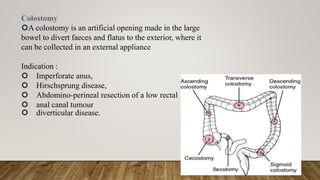
This document provides information on indications and construction of stomas. It defines a stoma as an artificial opening in the abdominal wall that connects the bowel or urinary tract to the outside environment. It describes different types of stomas based on duration (temporary or permanent) and anatomical location. Common indications for stomas include feeding, lavage, decompression, diversion, and exteriorization. Details are provided on constructing ileostomies and colostomies, including important considerations for stoma site selection and marking. Routine post-operative stoma care is also outlined.





























































![Basics of Stoma and Management care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/basicsofstomaandmanagement1-250417022629-8799f789-thumbnail.jpg?width=640&height=640&fit=bounds)

























