This document discusses biosafety levels (BSL) for handling pathogens in laboratories and provides examples of pathogens for each level. It also summarizes categories of public health threats (A, B, C), key indicators of potential bioterrorism, characteristics of bioterror agents, examples of criminal use of microbes, and the structure and function of the Laboratory Response Network for handling bioterrorism cases in the US. It provides overviews of several pathogenic bacteria and viruses of concern for bioterrorism, including anthrax, plague, tularemia, brucellosis, and viral hemorrhagic fevers.
biological weapons, an weapons which can kill many and that also by means of biology this may refer as silent killer as being describe in many science fiction movies like resident evil etc
Bioterrorism is using living organsims as weapons of mass destruction or to cause panic in population. it has existed since ancient times and yet pose a potential future threat. this compilation is not exhaustive and contains references at the end for further reading
biological weapons, an weapons which can kill many and that also by means of biology this may refer as silent killer as being describe in many science fiction movies like resident evil etc
Bioterrorism is using living organsims as weapons of mass destruction or to cause panic in population. it has existed since ancient times and yet pose a potential future threat. this compilation is not exhaustive and contains references at the end for further reading
This presentation focuses on a short history of bioterrorism, description, its advantages and disadvantages and organisms incorporated into weapons are also shown here.
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.
Medical Laboratory Scientist-microbiology summaryProtegeNithi
ASCP certified exam review. Microbiology basics for students taking Medical Laboratory Scientist exam. This is not comprehensive review. Some points to remember
Clinical chemistry review sheet for mlt certification and ascpDonna Kim
This is a fairly thorough without being bogged down with unnecessary detail study guide for Medical Laboratory Technician studying for the review and state exams
Acid Base
Carbohydrates
Lipids
Proteins
Amino Acids
Anthrax is a life-threatening infectious disease caused by Bacillus anthracis that normally affects animals, especially ruminants (such as goats, cattle, sheep, and horses). Anthrax can be transmitted to humans by contact with infected animals or their products.Anthrax cannot be spread directly from person to person, but a person's clothing and body may be contaminated with anthrax spores. Antibiotics often cure anthrax if it is diagnosed early. But many people don't know they have anthrax until it is too late to treat
Loboratory acquired infections & blood born pathogensAsmaraAslam1
This presentation includes the basic knowledge of Laboratory acquired infections & blood born pathogens with a lot of understandable knowledge and also how to use it properly. I hope all the finders liked it and also remember me in your precious Dua. Thank You!
“Microbial forensics” has been defined as “a scientific discipline dedicated to analyzing evidence
from a bioterrorism act, biocrime, or inadvertent microorganism/toxin release for attribution
purposes” (Budowle et al., 2003). This emerging discipline is still in the early stages of
development and faces substantial scientific challenges to provide a robust suite of technologies
for identifying the source of a biological threat agent and attributing a biothreat act to a particular
person or group. The unlawful use of biological agents poses substantial dangers to individuals,
public health, the environment, the economies of nations, and global peace. It also is likely that
scientific, political, and media-based controversy will surround any investigation of the alleged
use of a biological agent, and can be expected to affect significantly the role that scientific
information or evidence can play. For these reasons, building awareness of and capacity in
microbial forensics can assist in our understanding of what may have occurred during a biothreat
event, and international collaborations that engage the broader scientific and policy-making
communities are likely to strengthen our microbial forensics capabilities. One goal would be to
create a shared technical understanding of the possibilities—and limitations—of the scientific
bases for microbial forensics analysis._ NCBI
A biological attack, or bioterrorism, is the intentional release of viruses, bacteria, or other germs that can sicken or kill people, livestock, or crops. Bacillus anthracis, the bacteria that causes anthrax, is one of the most likely agents to be used in a biological attack.
This presentation describes tuberculosis with zoonotic significance. The presentation also includes data of disease burden, epidemiology, diagnosis, treatment regimes and control strategies.
OHH Unit 3 Biological and ergonomical hazards 1.pptABHINANDHKA1
Biological and ergonomical hazards in an occupation. ergonomics means rules of work. In this work is fit to the worker instead of fitting the worker to a job.
Biological agents are bacteria, Fungi, Prions and Virus etc. By implementing the hierarchy of control measures, it can be mitigated upto an optimal limit,
Similar to Microbiology - Agents of Bioterrorism (20)
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
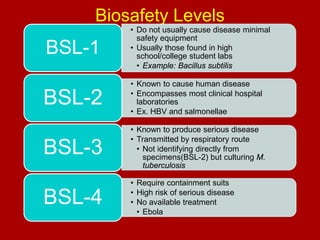
1. Biosafety Levels
BSL-1
• Do not usually cause disease minimal
safety equipment
• Usually those found in high
school/college student labs
• Example: Bacillus subtilis
BSL-2
• Known to cause human disease
• Encompasses most clinical hospital
laboratories
• Ex. HBV and salmonellae
BSL-3
• Known to produce serious disease
• Transmitted by respiratory route
• Not identifying directly from
specimens(BSL-2) but culturing M.
tuberculosis
BSL-4
• Require containment suits
• High risk of serious disease
• No available treatment
• Ebola
2. Public Health Preparedness
Three categories
Category A
• Greatest impact
Category B
Salmonella, ricin, E.coli O157:H7
Category C
• Less impact
Anthrax, hemorrhagic fevers
MDR-TB, hantavirus
See Table 30-1 for full list of examples
4. General Characteristics of Bioterror
Agents
Easily made
Mobile
Low skill required
Easy to transport
Transmission
Aerosol
Person-to-person spread
Resistant to decay
5. History of Criminal Use of Microbial
Agents
Salmonella
Anthrax spores
Sprayed onto salad bars in restaurants
Contaminated letters in NY, DC, and Florida
Ricin toxin
6. Laboratory Response Network (LRN)
Established in 1999
Community hospitals with microbiology
capabilities
Sentinel laboratories
• Must have BSL-2 capabilities
Five agents with protocols
–
–
–
–
–
B. anthracis
Y. pestis
F. tularensis
Brucella spp.
Etc.
7. Laboratory Response Network (LRN)
Reference laboratories
Perform confirmatory tests on several biothreat
agents
• State public health laboratories
• Department of defense medical center laboratories
National laboratories
Can perform complex forensic studies
Definitive characterization of biothreat agents
• CDC
• USAMRIID
• National Research Medical Center
9. Agents of Bioterror
Bacillus anthracis
Cutaneous anthrax
• Very few cases
Black eschar on skin
Gastrointestinal anthrax
• Ingestion of spores in contaminated
food
Inhalation anthrax
• Generally none unless bioterror or
lab accident
10. Agents of Bioterror
Specimen collection
Swabs from black eschar
Blood sample from inhalation and gastrointestinal
anthrax
• Colonies have medusa-head morphology
Nonhemolytic
13. Agents of Bioterror
Transmission
Bite of infected fleas
Handling contaminated materials
Inhaling aerosolized bacteria
Weaponized Y. pestis
Primarily pneumonic plague
• Person-to-person transmission
14. Agents of Bioterror
Symptoms
Fever, chills, headache, malaise
Buboes
• Inflammation of the lymph node causing swelling
Bacteria disseminate and cause DIC
– Results in gangrene in fingers and nose
15. Agents of Bioterror
Direct examination and culture
Plump gram-negative rods
Bipolar staining
• Safety pin appearance
16. Agents of Bioterror
Francisella tularensis
BSL-3 pathogen
Zoonotic disease
Infectious dose
• As low as 10 organisms
Ulceroglandular tularemia
Skin infection
• Bite of infected insect
• Handling infectious materials
18. Agents of Bioterror
Clinical manifestations
Symptoms
• Fever with chills
• Headaches
• Cough
• Chest pain
• Lesions at site of entry
Occasionally respiratory disease
19. Agents of Bioterror
Brucella spp.
Small gram-negative pleomorphic aerobic
coccobacilli
• Brucella melitensis
• Brucella suis
• Brucella abortus
Mostly eliminated in the United States
• BSL-3 containment required
Transmission
• Breaks in skin
• Ingestion of food products
• Aerosols in laboratory conditions
20. Agents of Bioterror (Cont’d)
Symptoms
Can persist for months
Malaise, night sweats, relapsing fever, chills,
myalgia
• Requires 5-35 days of incubation before symptoms
Most recover without treatment
Previous use as a biologic weapon
21. Agents of Bioterror (Cont’d)
Burkholderia species
B. mallei
• Glanders
B. pseudomallei
• Melioidosis
Symptoms
• Fever, myalgia, headache, and chest pain
Caused by cutaneous lesions, bloodstream infections,
pneumonia
22. Agents of Bioterror (Cont’d)
Coxiella burnetii
Causative agent of Q fever (Query fever)
Reservoirs
• Cattle, sheep, goats, dogs, cats, deer, fowl, and humans
• Exposure in vet or animal handlers
Transmission
• Urine, milk, feces, tissues, and fluids expelled during
birth
• Incubation period 2-3 weeks
23. Agents of Bioterror
Smallpox
Two major forms
• Variola major
30% mortality in unvaccinated
3% in vaccinated
• Variola minor
Similar but much less severe disease
25. Agents of Bioterror
Viral hemorrhagic fevers
Ebola, Marburg, Lassa fever, Crimean-Congo, Rift
Valley fever, Hantavirus
Transmission
Direct contact
Urine, semen
26. Agents of Bioterror (Cont’d)
Clinical manifestations
Incubation period 2 to 3 weeks
Fever, rash, myalgia, arthralgia, nausea,
conjunctivitis, diarrhea, and CNS symptoms
Bleeding, DIC, hemorrhage of mucous
membranes
• Some have high mortality rates