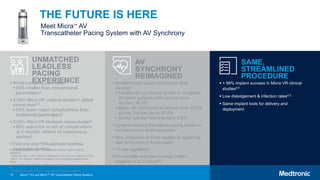
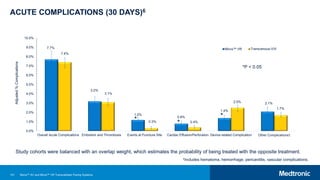
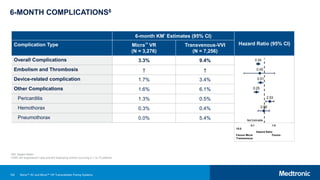
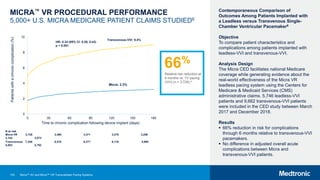
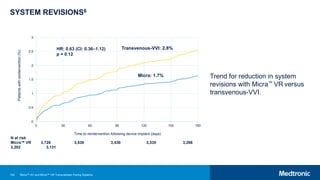
The document introduces the micra AV and micra VR transcatheter pacing systems, highlighting their leadless design as the world's smallest pacemakers, which offer a 93% reduction in size compared to traditional devices and 63% fewer major complications. It emphasizes the enhanced functionality of the micra AV system, including AV synchrony for more effective pacing, and provides data supporting its clinical efficacy, showing a 66% reduction in complication risk compared to transvenous devices. Additionally, it notes the success rates of implantation and low rates of dislodgment and infection, presenting leadless pacing as a significant advancement in cardiac care.






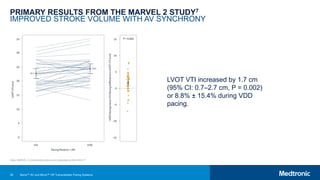
![48
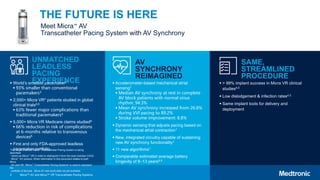
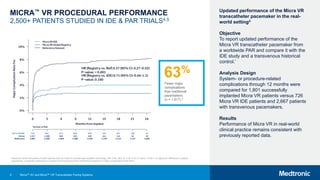
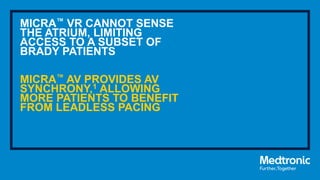
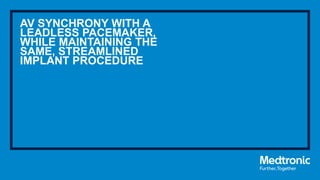
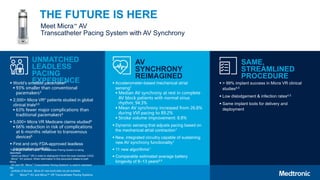
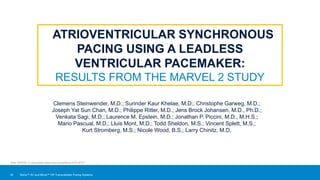
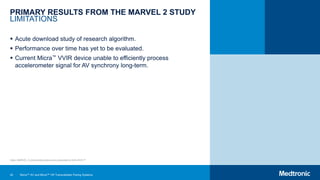
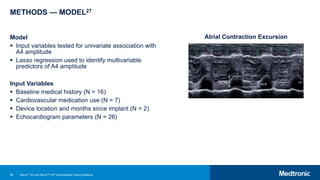
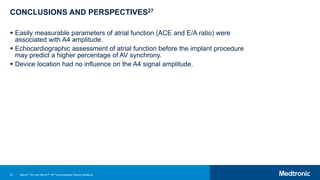
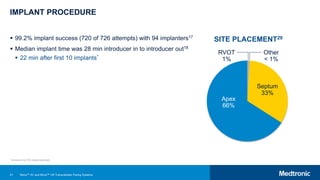
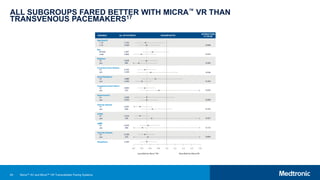
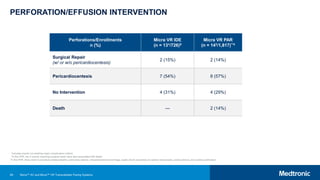
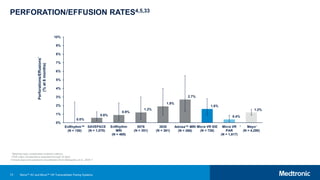
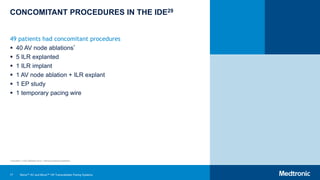
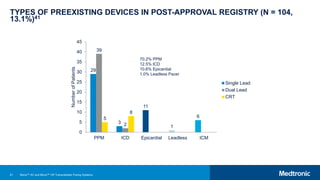
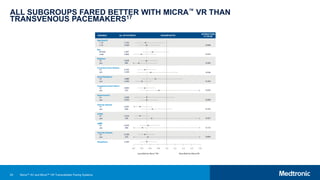
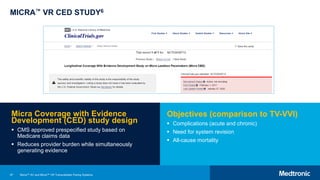
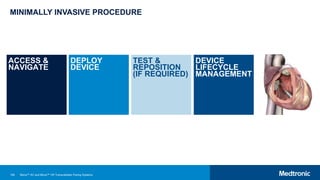
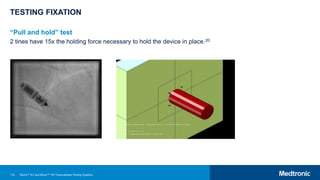
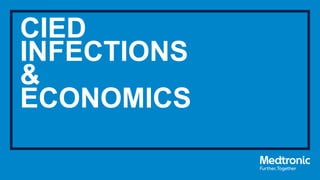
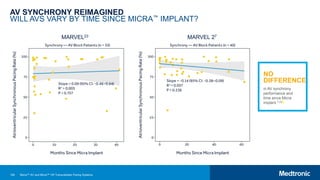
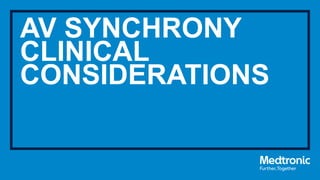
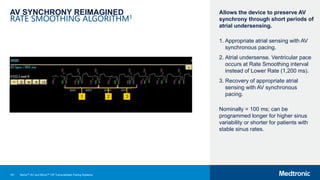
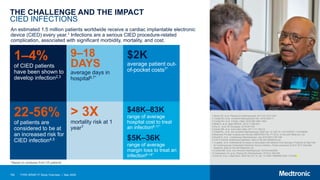
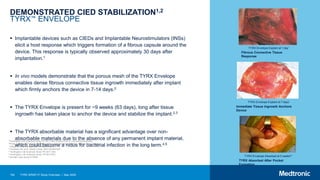
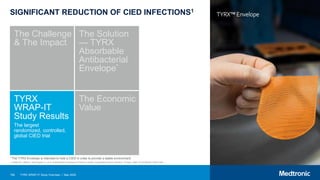
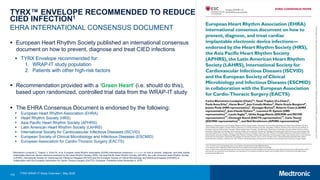
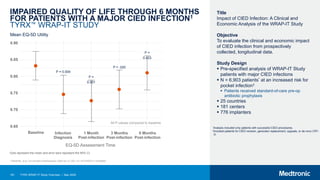
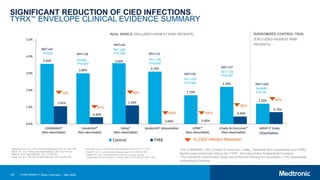
RESULTS27
Variable Type Variables Summary
Univariate Models Multivariable Model
β (95% CI) P-value R2 β (95% CI) P-value
Baseline and
Medical History
Male 54.7% -0.57 (-1.25–0.10) 0.099 0.04
Systolic blood pressure 137 ± 20 [92–176] 0.02 (0.00–0.04) 0.036 0.07
History of atrial arrhythmias 15.6% -0.81 (-1.73–0.11) 0.089 0.05
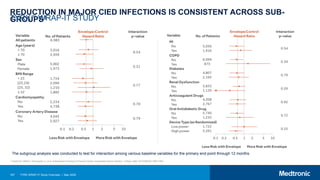
CABG 12.5% -1.41 (-2.38 to -0.44) 0.006 0.12 -1.01 (-1.8 to -0.13) 0.025
Prior valve surgery 21.9% -0.80 (-1.60–0.00) 0.056 0.06
Echocardiography
4-chamber TR jet area 3 ± 2 [0–12] -0.15 (-0.32–0.01) 0.077 0.05
LV ejection fraction 54 ± 4 [40–61] 0.21 (0.02–0.39) 0.030 0.08
LA end-diastolic volume 52 ± 19 [19–92] -0.12 (-0.25–0.02) 0.088 0.05
LA end-systolic volume 25 ± 10 [8–44] -0.13 (-0.25–0.00) 0.055 0.06
LA ejection fraction 53.23 ± 3.99 [46.15–63.04] 0.13 (-0.01–0.28) 0.070 0.05
E/A (mitral valve) 1.18 ± 0.62 [0.48–3.43] -0.25 (-0.39 to -0.10) 0.002 0.15 -0.13 (-0.28–0.02) 0.092
RV TAPSE 2.4 ± 0.5 [1.4–3.4] 0.23 (0.10–0.37) 0.001 0.15
Atrial contraction excursion
(ACE)
1.0 ± 0.2 [0.5–1.7] 0.34 (0.18–0.49) < 0.001 0.23 0.26 (0.11–0.42) 0.001
E/e’ 12.67 ± 6.27 [4.10–31.41] -0.12 (-0.27–0.02) 0.097 0.05
e/a’ lateral 1.25 ± 0.85 [0.47–4.57] -0.19 (-0.34 to -0.03) 0.024 0.08
e’/a’ septal 1.27 ± 1.01 [0.45–5.00] -0.16 (-0.31 to -0.01) 0.039 0.07
e’/a’ average 1.18 ± 0.66 [0.54–3.90] -0.24 (-0.41 to -0.08) 0.005 0.12
Atrial strain Ԑa 8.3 ± 4.4 [1.2–21.6] 0.16 (0.01–0.32) 0.045 0.06 0.11 (-0.03–0.24) 0.117
Micra™ AV and Micra™ VR Transcatheter Pacing Systems](https://image.slidesharecdn.com/micraandtyrxcustomerpresentation1-240629151400-72fd877b/85/Micra-and-Tyrx-Customer-Presentation-1-pptx-48-320.jpg)









![129
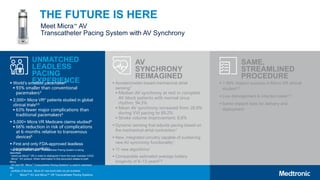
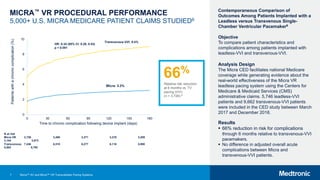
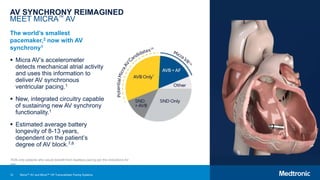
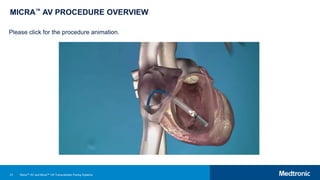
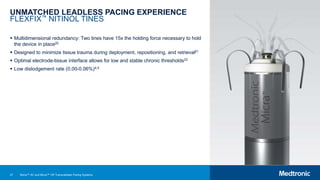
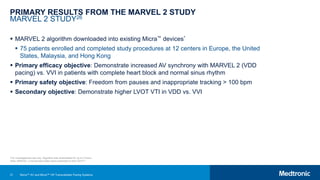
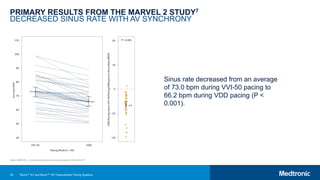
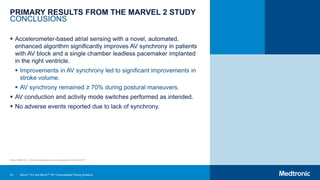
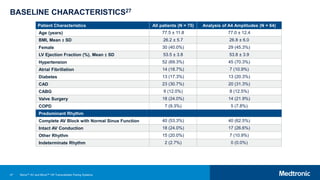
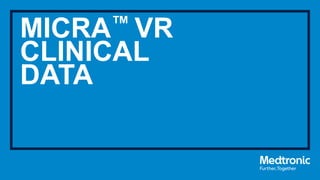
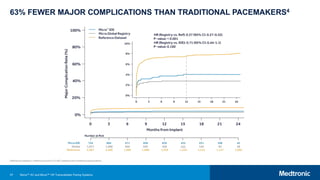
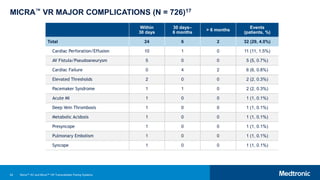
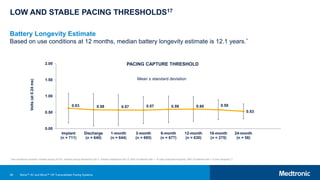
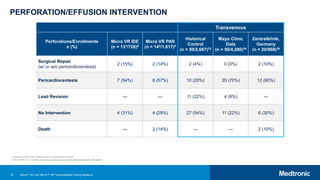
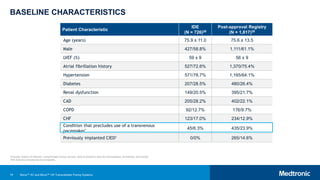
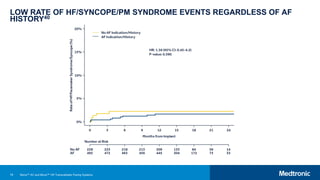
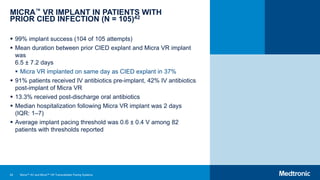
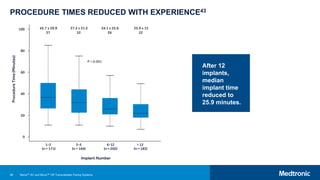
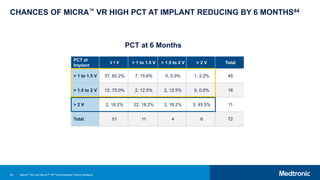
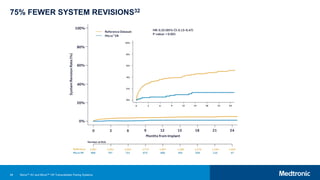
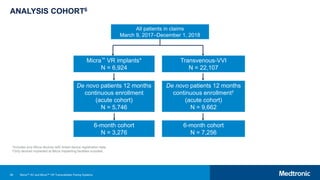
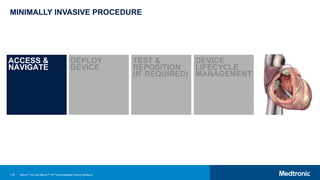
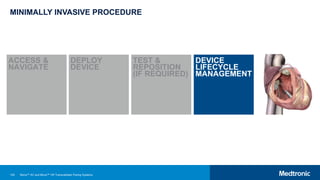
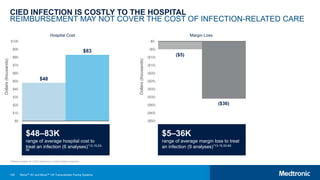
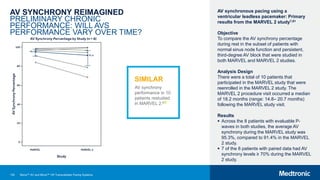
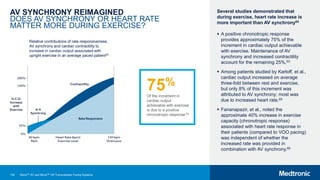
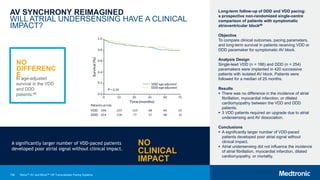
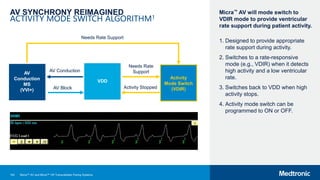
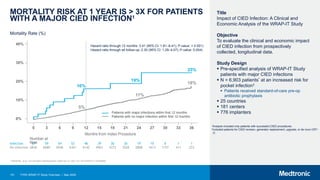
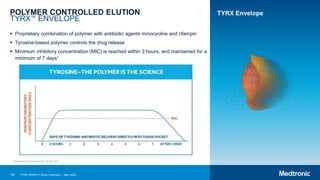
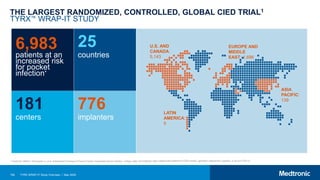
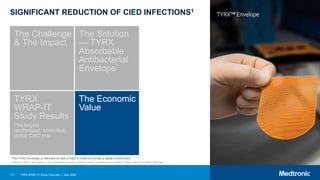
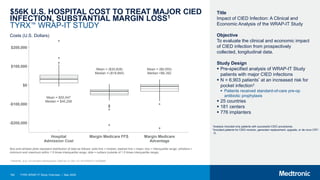
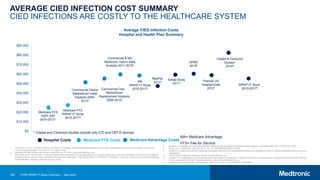
AV SYNCHRONY REIMAGINED
PRELIMINARY CHRONIC PERFORMANCE:
WILL AVS PERFORMANCE VARY OVER TIME?
Closed circles represent A4 amplitudes at visit
1.
Open circles represent A4 amplitudes at visit 2.
NO
DIFFERENC
E
In AV synchrony
performance in
patients restudied
after 6 months.24
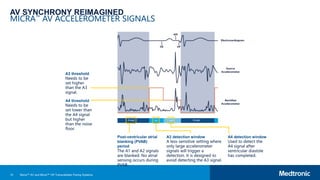
Behavior of leadless AV synchronous pacing
during atrial arrhythmias and stability of the
atrial signals over time-Results of the
MARVEL Evolve subanalysis24
Methods
This prospective single-center study compared
AV synchrony and accelerometer signals at two
visits ≥ 6 months apart. Custom software was
temporarily downloaded into the Micra™ at each
visit and AVS was measured during 30 minutes
at rest.
Results
9 patients from the MARVEL study were
enrolled. Micra was implanted for 6.0 ± 6.4
months. The mean interval between visits was
7.1 ± 0.6 months. 7 patients had normal sinus
node function between both visits and were
included in a paired analysis. Both
accelerometer signal amplitude (visit 2–visit 1 =
1.4 mG; 95% confidence interval [CI] [-25.8 to
28.4 mG]; P = 0.933) and AVS (visit 1: 90.8%,
95% CI [72.4, 97.4] and visit 2: 91.4%, 95% CI
[63.8, 98.5]; P = 0.740) remained stable.
Conclusion
Accelerometer signals amplitude and
performance of AVS pacing were stable over
time.
Micra™ AV and Micra™ VR Transcatheter Pacing Systems](https://image.slidesharecdn.com/micraandtyrxcustomerpresentation1-240629151400-72fd877b/85/Micra-and-Tyrx-Customer-Presentation-1-pptx-129-320.jpg)
![143
REFERENCES
1 Medtronic Micra™ AV MC1AVR1 Reference Manual. January 2020.
2 Nippoldt D, Whiting J. Micra Transcatheter Pacing System Device Volume Characterization Comparison. November
2014. Medtronic data on file.
3 Williams E, Whiting J. Micra Transcatheter Pacing System Size Comparison. November 2014. Medtronic data on
file.
4 El-Chami MF, Al-Samadi F, Clementy N, et al. Updated performance of the Micra transcatheter pacemaker in the
real
world setting: A comparison to the investigational study and a transvenous historical control. Heart Rhythm.
December
2018;15(12):1800-1807.
5 Reynolds D, Duray GZ, Omar R, et al. A Leadless Intracardiac Transcatheter Pacing System. N Engl J Med.
February 11,
2016;374(6):533-541.
6 Picinni JP, et al. Comparison of Outcomes Among Patients Implanted with a Tined, Leadless Versus Transvenous
Single-Chamber Ventricular Pacemaker in the Novel Micra Coverage with Evidence Development Study. Heart
Rhythm.
2020 May 08. doi: 10.1016/j.hrthm.2020.04.044. [Epub ahead of print].
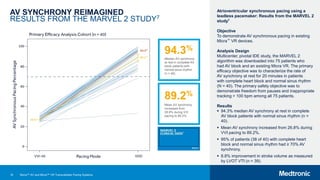
7 Steinwender C, Khelae SK, Garweg C, et al. Atrioventricular synchronous pacing using a leadless ventricular
pacemaker:
Results from the MARVEL 2 Study. JACC Clin Electrophysiol. 2020;6(1):94-106.
8 Pender J, Whiting J. Micra AV Battery Longevity. January 2020. Medtronic data on file.
9 Medtronic Micra™ AV MC1AVR1 Device Manual. January 2020.
10 Cantillon DJ, Exner DV, Badie N, et al. Complications and Health Care Costs Associated With Transvenous Cardiac
Pacemakers in a Nationwide Assessment. JACC Clin Electrophysiol. November 2017;3(11):1296-1305.
11 Udo EO, Zuithoff NP, van Hemel NM et al. Incidence and predictors of short- and long-term complications in
pacemaker
therapy: the FOLLOWPACE study. Heart Rhythm. May 2012;9(5):728-735.
12 Tarakji KG, Wilkoff BL. Management of cardiac implantable electronic device infections: the challenges of
understanding
the scope of the problem and its associated mortality. Expert Rev Cardiovasc Ther. May 2013;11(5):607-616.
13 Sohail MR, Henrikson CA, Braid-Forbes MJ, Forbes KF, Lerner DJ. Mortality and cost associated with
cardiovascular
implantable electronic device infections. Arch Intern Med. November 14, 2011;171(20):1821-1828.
14 Sohail MR, Eby EL, Ryan MP, Gunnarsson C, Wright LA, Greenspon AJ. Incidence, Treatment Intensity, and
Incremental
Annual Expenditures for Patients Experiencing a Cardiac Implantable Electronic Device Infection: Evidence From a
Large
US Payer Database 1-Year Post Implantation. Circ Arrhythm Electrophysiol. August 2016;9(8).
15 Wilkoff BL, et al. Impact of CIED Infection: A Clinical and Economic Analysis of the Wrap-It Study. Presentation
Su3088
at AHA Scientific Sessions 2019; Philadelphia, PA.
16 Medtronic Micra™ MC1VR01 Clinician Manual. October 2016.
17 Duray GZ, Ritter P, El-Chami M, et al. Long-term performance of a transcatheter pacing system: 12-Month results
from
Pacemaker.
IEEE Trans Biomed Eng. September 2015;62(9):2316-2323.
21 Eggen M. FlexFix Tine Design. April 2015. Medtronic data on file.
22 Bonner M, Eggen M, Haddad T, Sheldon T, Williams E. Early Performance and Safety of the Micra Transcatheter
Pacemaker in Pigs. Pacing Clin Electrophysiol. November 2015;38(11):1248-1259.
23 Chinitz L, Ritter P, Khelae SK, et al. Accelerometer-based atrioventricular synchronous pacing with a ventricular
leadless pacemaker: Results from the Micra atrioventricular feasibility studies. Heart Rhythm. September
2018;15(9):1363-1371.
24 Garweg C, Splett V, Sheldon TJ, et al. Behavior of leadless AV synchronous pacing during atrial arrhythmias and
stability
of the atrial signals over time-Results of the MARVEL Evolve subanalysis. Pacing Clin Electrophysiol. March
2019;42(3):381-387.
25 Chinitz LA, et al. AV Synchronous Pacing Using a Ventricular Leadless Pacemaker: Primary Results from the
MARVEL 2
Study. Presented at AHA 2019; Philadelphia, PA.
26 Micra Atrial TRacking Using A Ventricular AccELerometer 2 (MARVEL2). Clinical trial identifier NCT03752151.
Available
at: https://clinicaltrials.gov/ct2/show/NCT03752151. Accessed December 3, 2019.
27 Garweg C, et al. Predictors of Accelerometer-Based Atrial Detection in a Leadless Ventricular Pacemaker. Heart
Rhythm. 2020;17(5S):S12.
28 Kirkfeldt RE, Johansen JB, Nohr EA, Jørgensen OD, Nielsen JC. Complications after cardiac implantable electronic
device implantations: an analysis of a complete, nationwide cohort in Denmark. Eur Heart J. May 2014;35(18):
1186-1194.
29 Nesse H. Micra Clinical Evidence from IDE Trial and Post-Approval Registry. May 2018. Medtronic data on file.
30 Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of
Cardiac
Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on
Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of
Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for
Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. May 27, 2008;51(21):e1-e62.
31 European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, et al. ACC/AHA/ESC 2006 guidelines for
management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the
American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology
Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With
Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol. September 5, 2006;48(5):
e247-e346.
32 Grubman E, Ritter P, Ellis CR, et al. To retrieve, or not to retrieve: System revisions with the Micra transcatheter
pacemaker. Heart Rhythm. December 2017;14(12):1801-1806.
33 Medtronic Micra FDA Panel Pack.
34 Mahapatra S, Bybee KA, Bunch TJ, et al. Incidence and predictors of cardiac perforation after permanent
pacemaker
placement. Heart Rhythm. September 2005;2(9):907-911.
35 Ohlow MA, Lauer B, Brunelli M, Geller JC. Incidence and predictors of pericardial effusion after permanent heart
Micra™ AV and Micra™ VR Transcatheter Pacing Systems](https://image.slidesharecdn.com/micraandtyrxcustomerpresentation1-240629151400-72fd877b/85/Micra-and-Tyrx-Customer-Presentation-1-pptx-143-320.jpg)






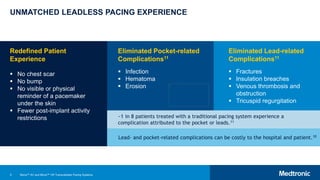
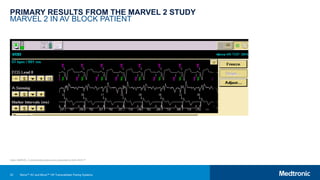
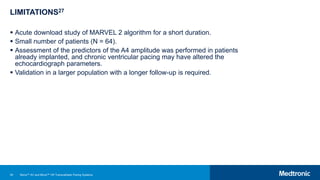
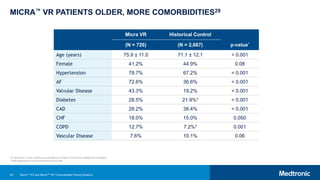
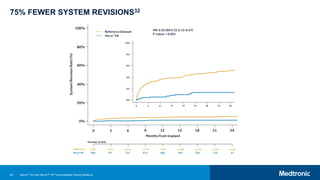
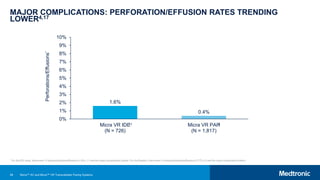
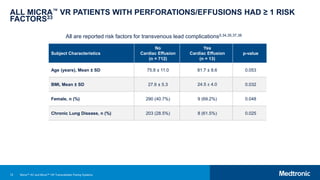
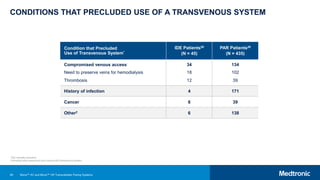
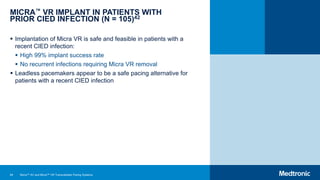
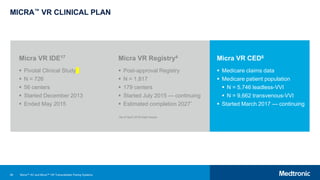
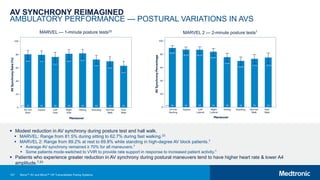
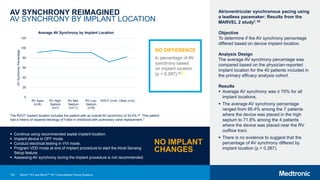
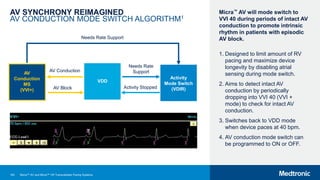
![178 TYRX WRAP-IT Study Overview | May 2020
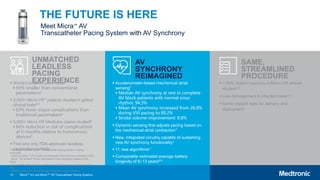
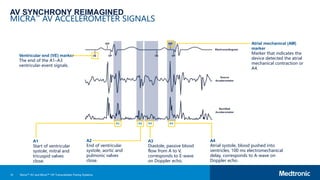
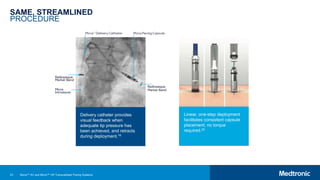
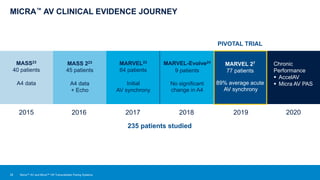
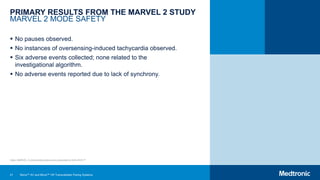
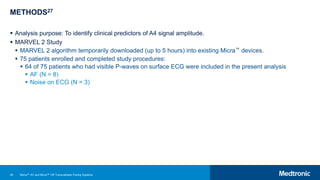
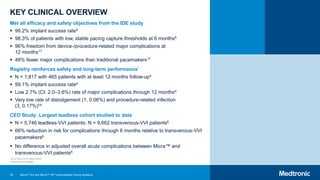
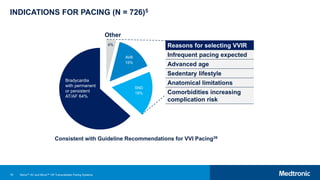
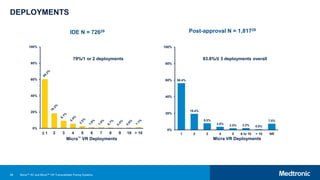
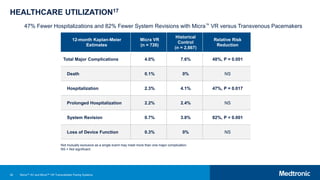
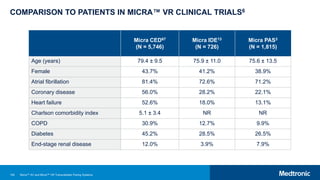
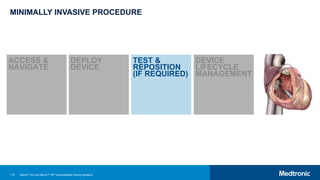
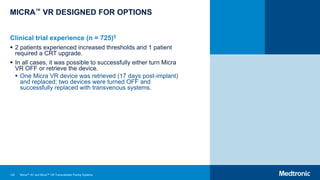
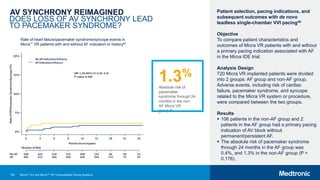
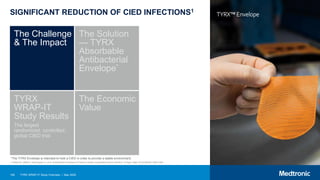
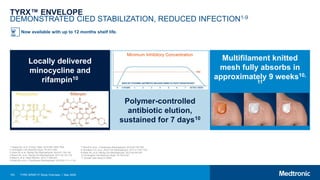
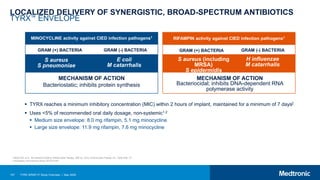
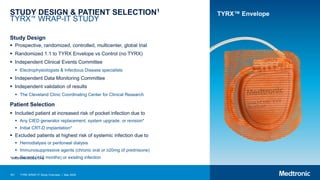
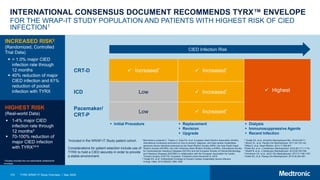
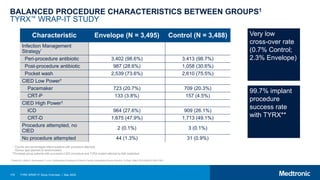
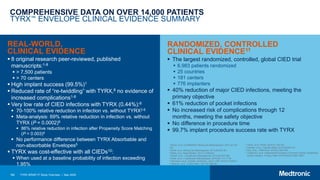
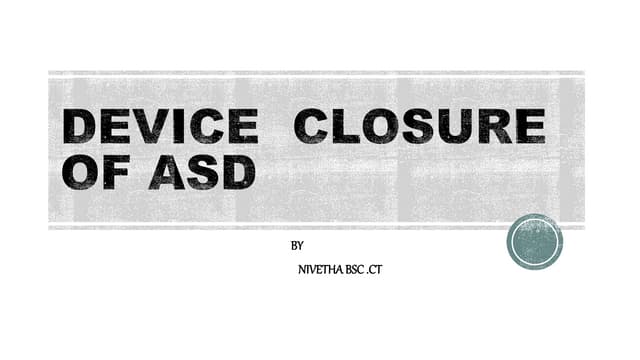
BASELINE CHARACTERISTICS BETWEEN GROUPS1
TYRX™ WRAP-IT STUDY
Characteristic
Envelope
(N = 3,495)
Control
(N = 3,488)
Age, (years) [Mean ± SD] 70.0 ± 12.6 70.1 ± 12.4
Female (%) 997 (28.6%) 976 (28.0%)
BMI (%) [Mean ± SD] 29.1 ± 6.1 29.2 ± 6.3
Diabetes 1,080 (30.9%) 1,085 (31.1%)
Renal dysfunction 585 (16.8%) 554 (15.9%)
Baseline Medications
Antiplatelets 2,007 (57.5%) 1,972 (56.6%)
Anticoagulants 1,377 (39.5%) 1,390 (39.9%)
Antibiotics 36 (1.0%) 37 (1.1%)
Immunosuppressive* 48 (1.4%) 85 (2.4%)
Insulin 348 (10.0%) 375 (10.8%)
Oral antidiabetic 615 (17.6%) 620 (17.8%)
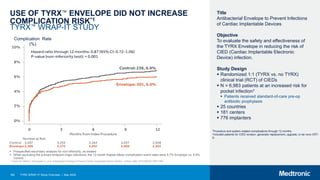
*No significant differences between groups except for the use of immunosuppressive agents (p=0.001); standardized difference does not suggest imbalance
1 Tarakji KG, Mittal S, Kennergren C, et al. Antibacterial Envelope to Prevent Cardiac Implantable Device Infection. N Engl J Med. 2019;380(20):1895-1905.](https://image.slidesharecdn.com/micraandtyrxcustomerpresentation1-240629151400-72fd877b/85/Micra-and-Tyrx-Customer-Presentation-1-pptx-178-320.jpg)



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





