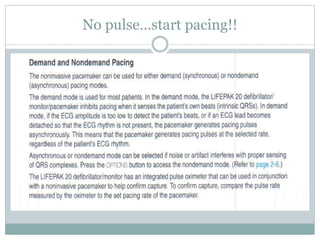
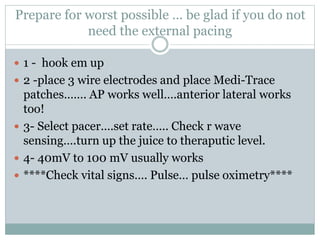
Noninvasive pacing is used for emergency treatment of symptomatic bradycardia. Electrical current is passed from an external pulse generator via electrodes placed on the chest to pace the heart. It can be initiated by various medical providers with minimal training. It is less expensive than invasive pacing and useful for patients at risk of infection or bleeding. However, it causes discomfort as current must pass through the chest wall and causes cutaneous and skeletal muscle stimulation.