Downloaded 200 times

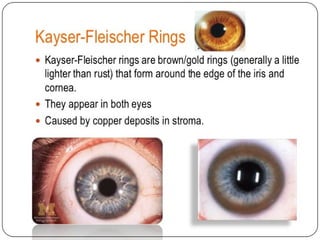

1. Copper and copper compounds like copper sulfate and copper subacetate are toxic heavy metals that can cause acute and chronic poisoning through ingestion, inhalation, or skin exposure. 2. Acute copper poisoning causes gastrointestinal symptoms like vomiting and diarrhea as well as liver and kidney damage. Chronic poisoning can result in conditions like anemia, bronchitis, and corneal ulcers. 3. Iron and thallium are also toxic heavy metals that can cause multiple organ damage and even death in acute overdoses. Their absorption is followed by stages of toxicity affecting the gastrointestinal tract, liver, kidneys, and other organs. 4. Potassium permanganate is a toxic compound of manganese that



















































































![Role of Forensic Pathologists in Mass Aviation Disasters[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/roleofforensicpathologistsinmassaviationdisasters1-231108070849-16463557-thumbnail.jpg?width=640&height=640&fit=bounds)





















