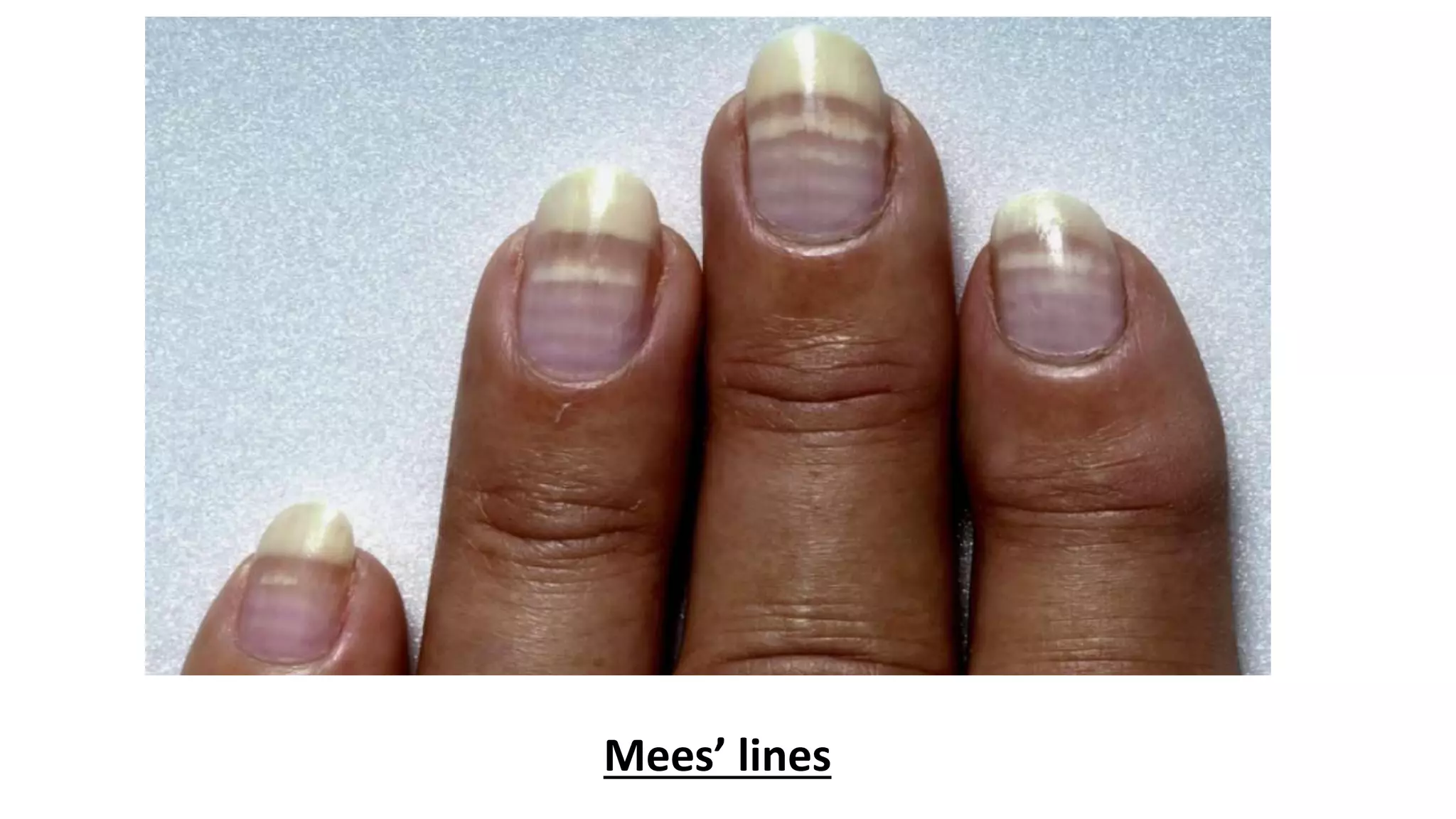
Heavy metal poisoning can involve multiple systems and be caused by various metals like arsenic, lead, mercury, and copper. Arsenic poisoning presents with gastrointestinal symptoms like vomiting and diarrhea as well as skin lesions. Lead poisoning commonly affects the nervous system causing issues like decreased IQ and hyperactivity. Mercury poisoning can cause pulmonary toxicity and kidney damage. Copper poisoning results in liver injury and haemolysis. Diagnosis involves measuring metal levels in blood and urine. Treatment focuses on decontamination, chelation therapy, and supportive care.