Downloaded 274 times
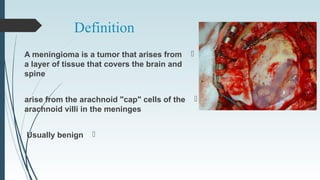
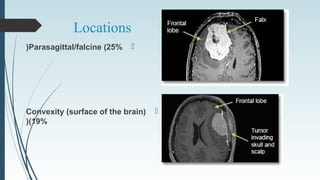
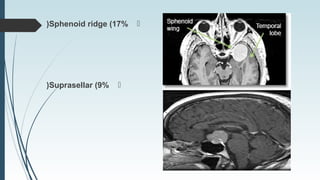
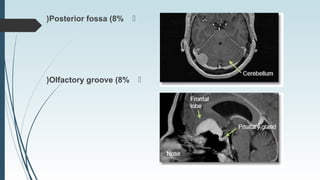
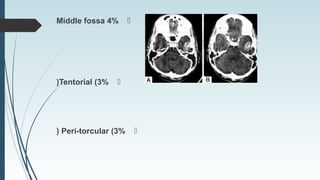





A meningioma is a typically benign tumor that arises from tissue covering the brain and spine, more common in women and associated with factors like radiation and cell phone use. Symptoms can vary from seizures to headaches and visual defects depending on the tumor's location, with treatment options including observation, surgical resection, and minimally invasive techniques. Histological grading categorizes these tumors into benign, atypical, and anaplastic, influencing the treatment approach.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









