Downloaded 287 times
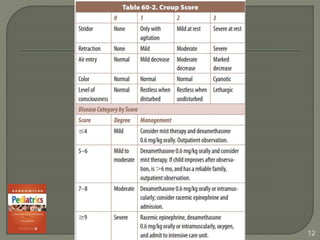


Croup is a condition characterized by a bark-like cough, often caused by viral infections, particularly parainfluenza viruses, and is most common in children aged 3 months to 5 years. Treatment primarily involves airway management and steroids like dexamethasone, while nebulized epinephrine may be used for moderate to severe cases. Antibiotics are not indicated, and supportive care is key, as symptoms typically resolve within a week.













































































