Downloaded 30 times
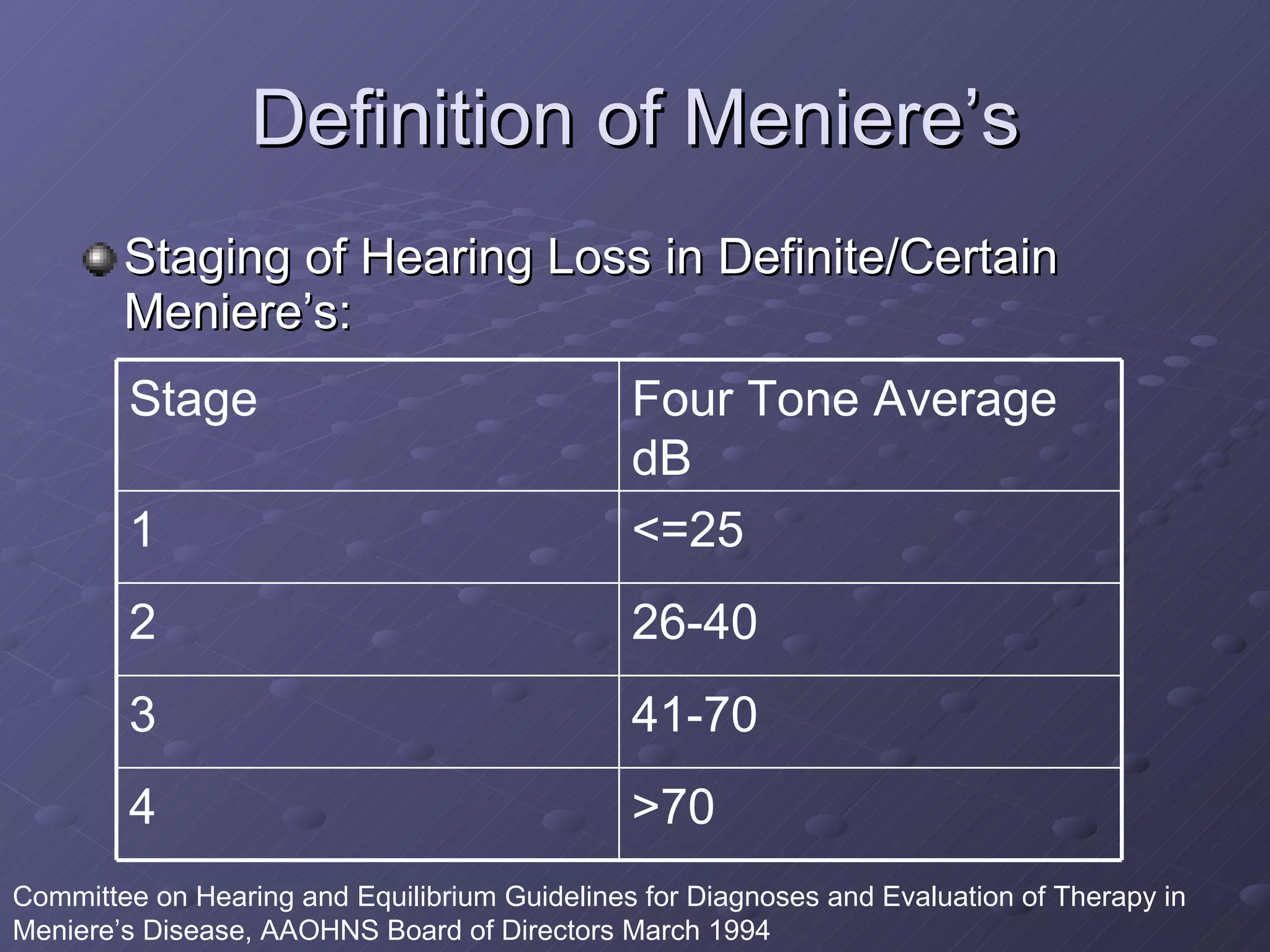
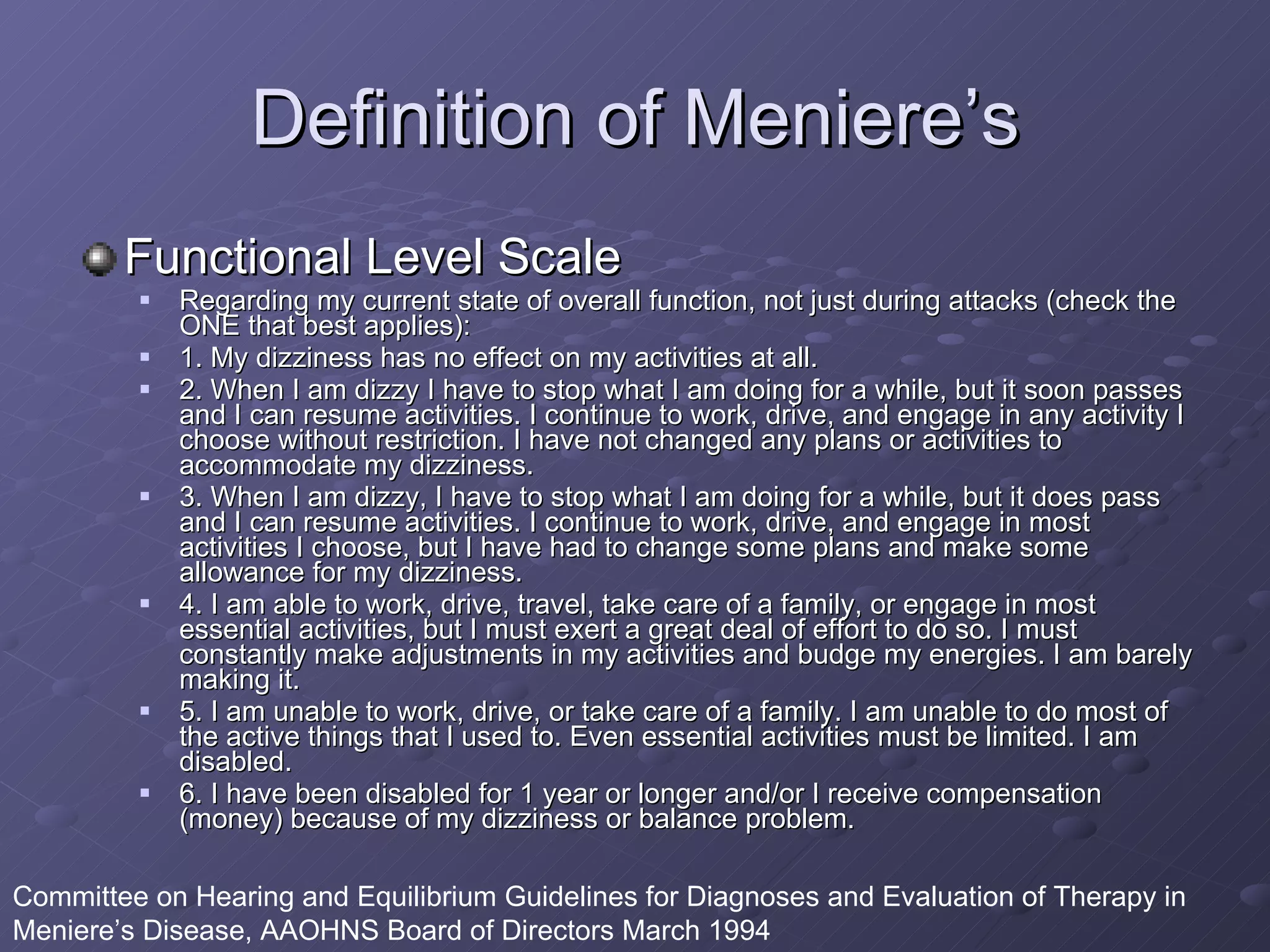
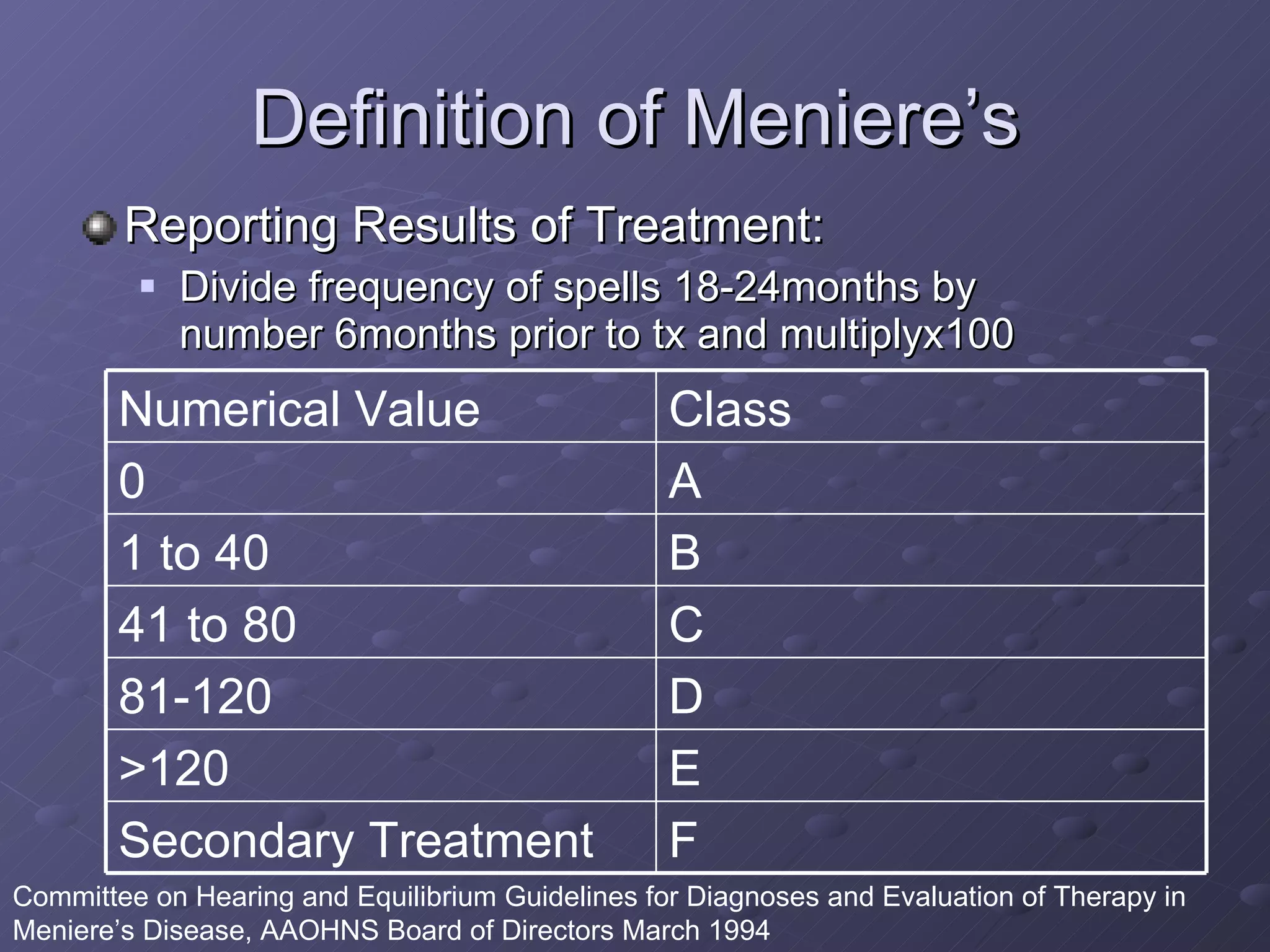
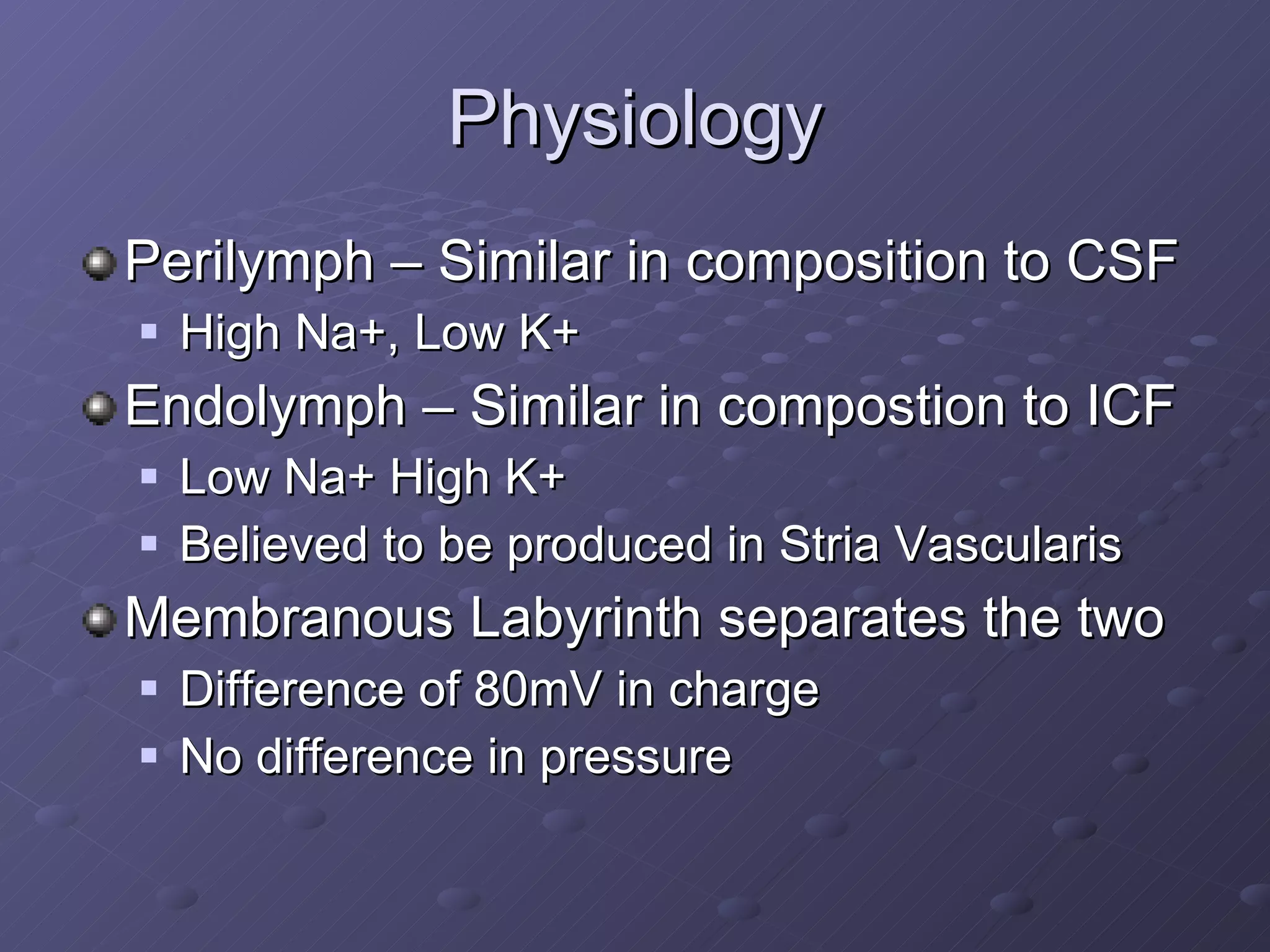

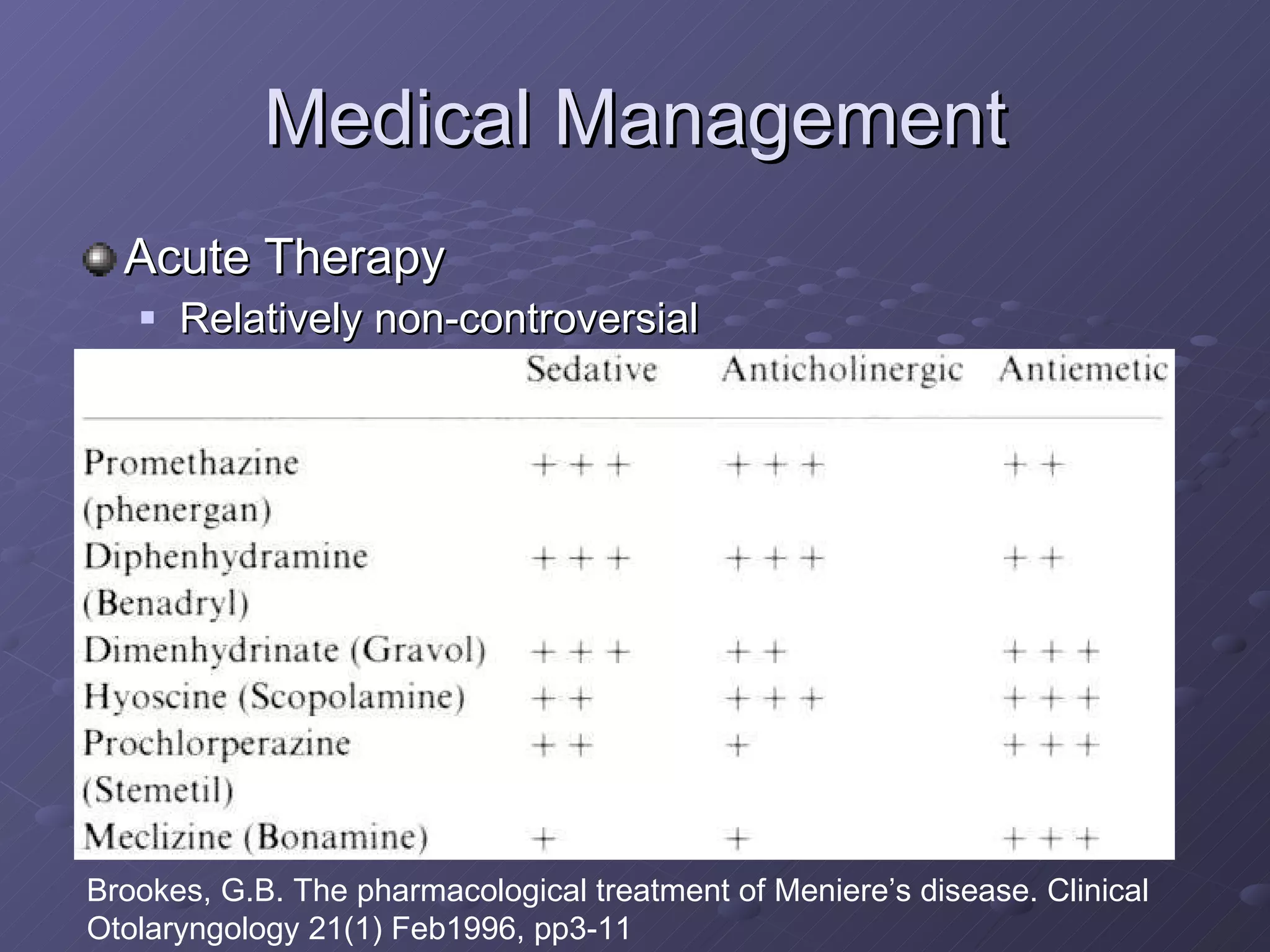


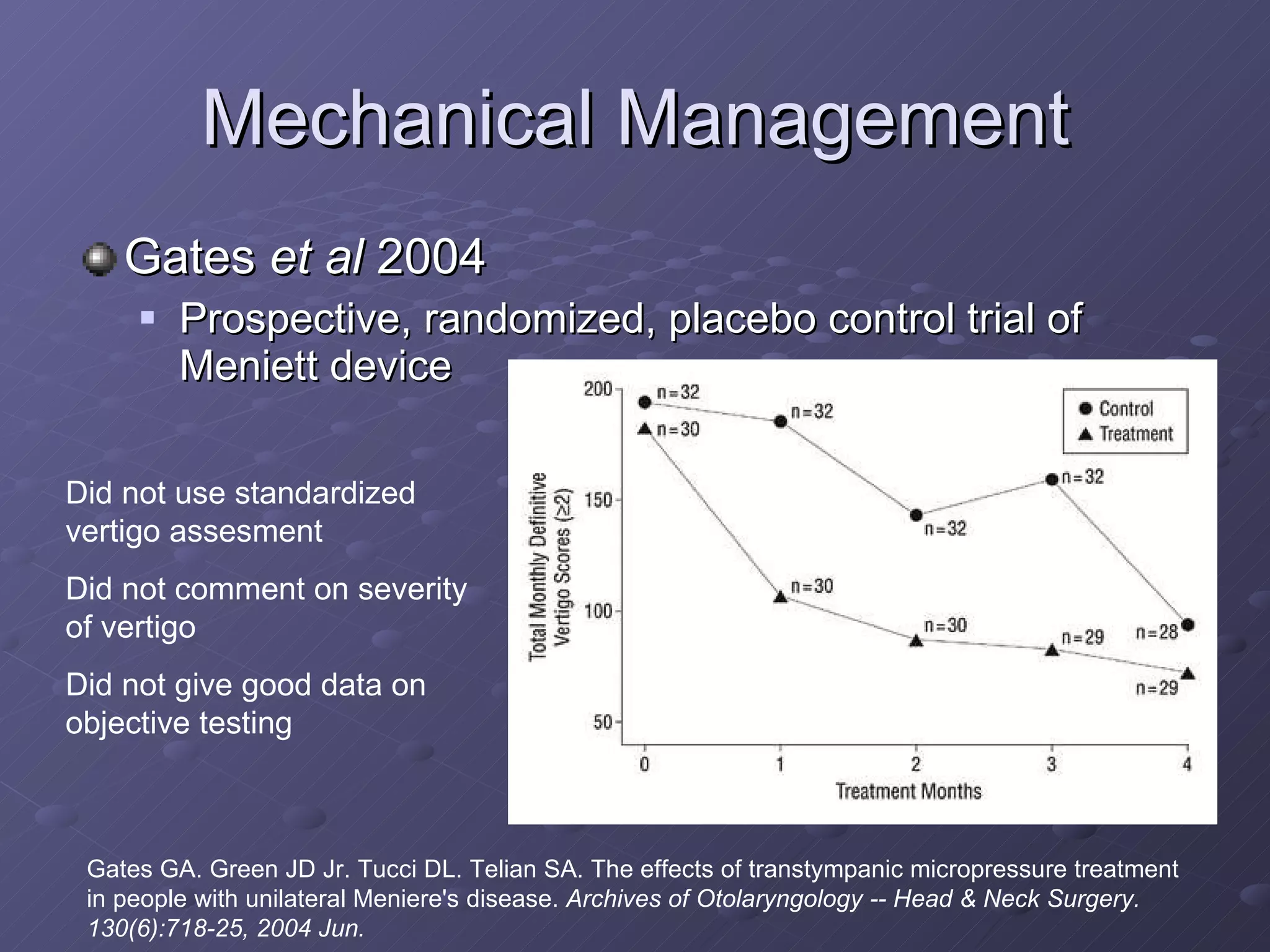



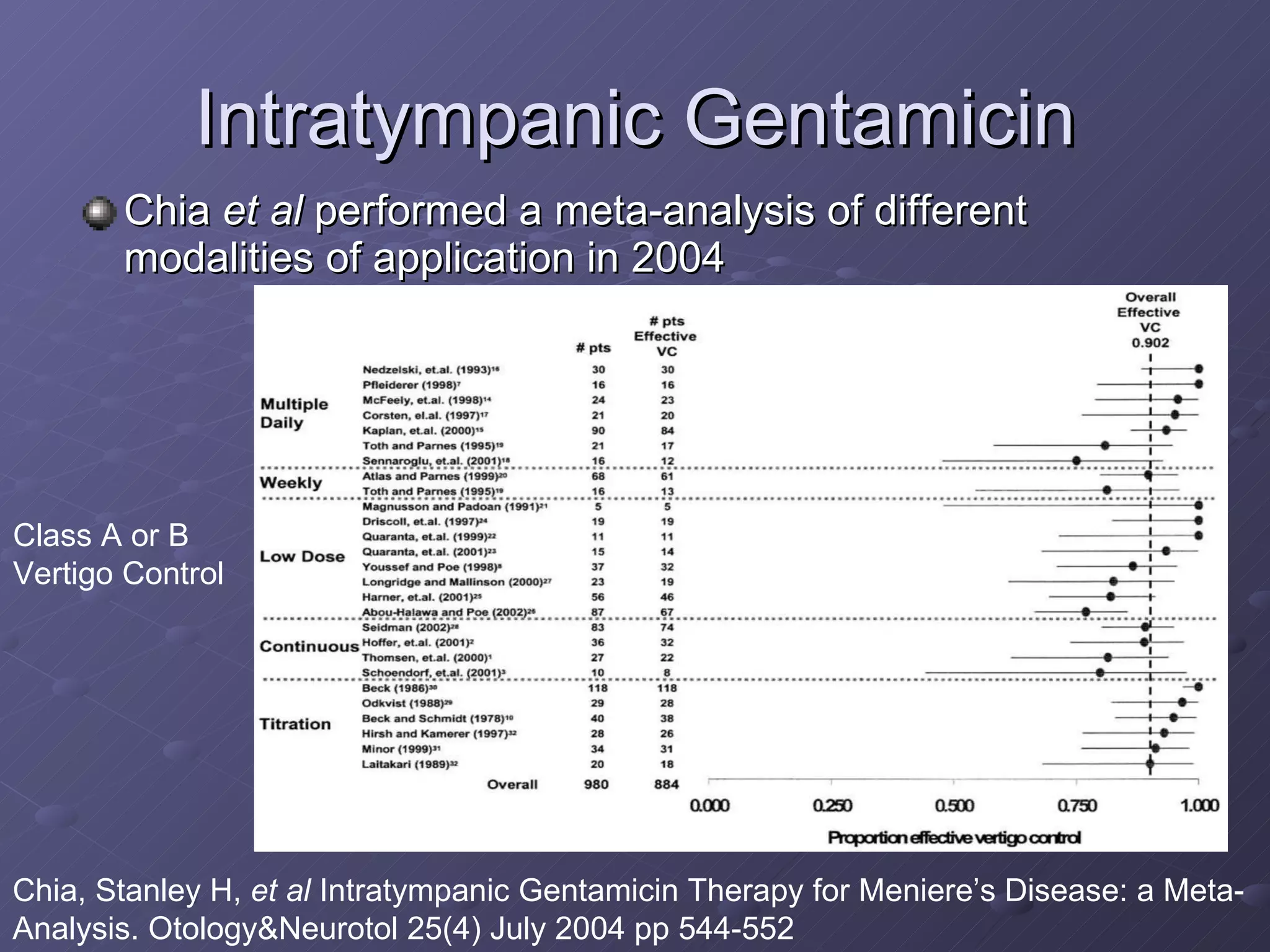




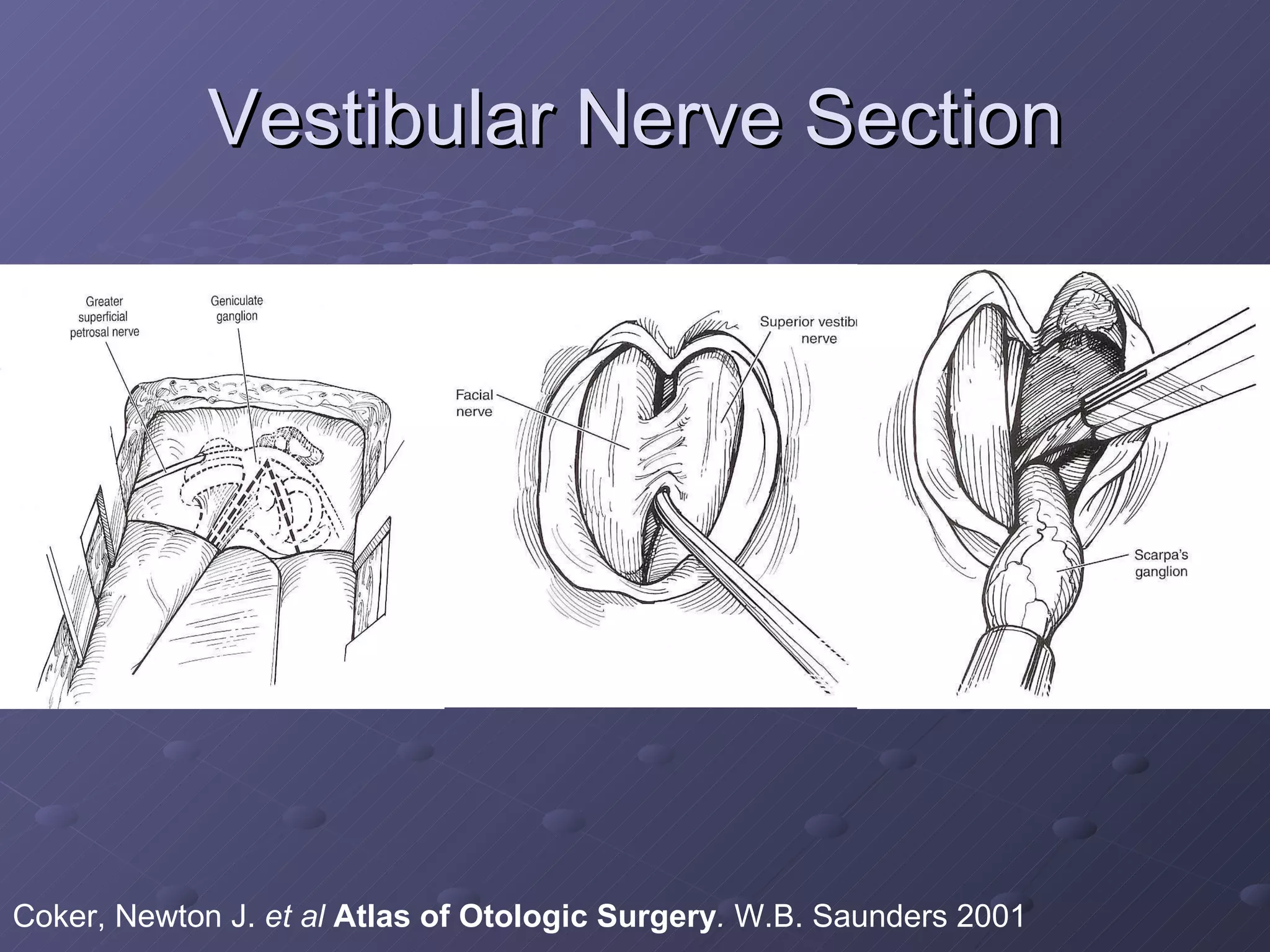
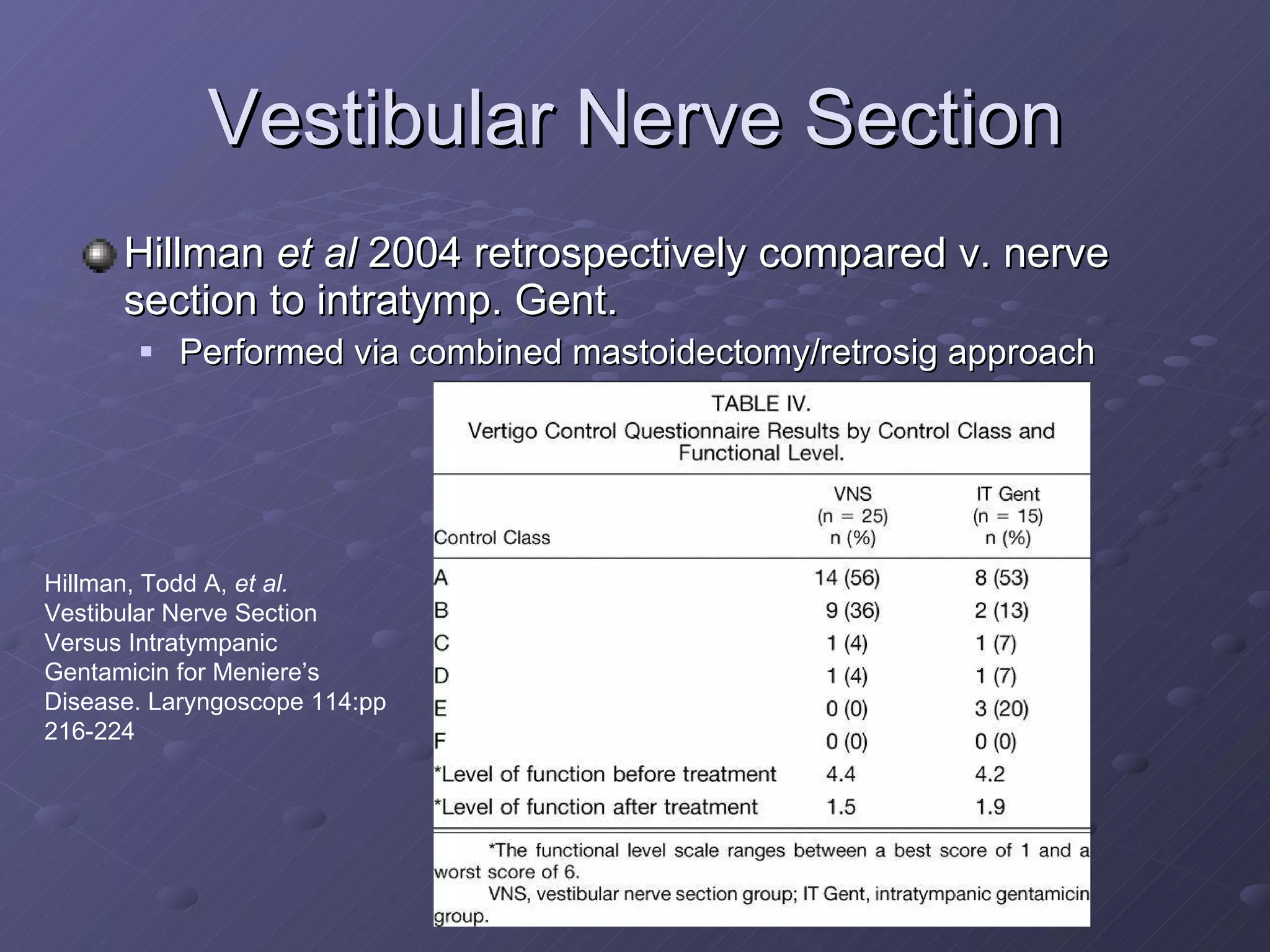
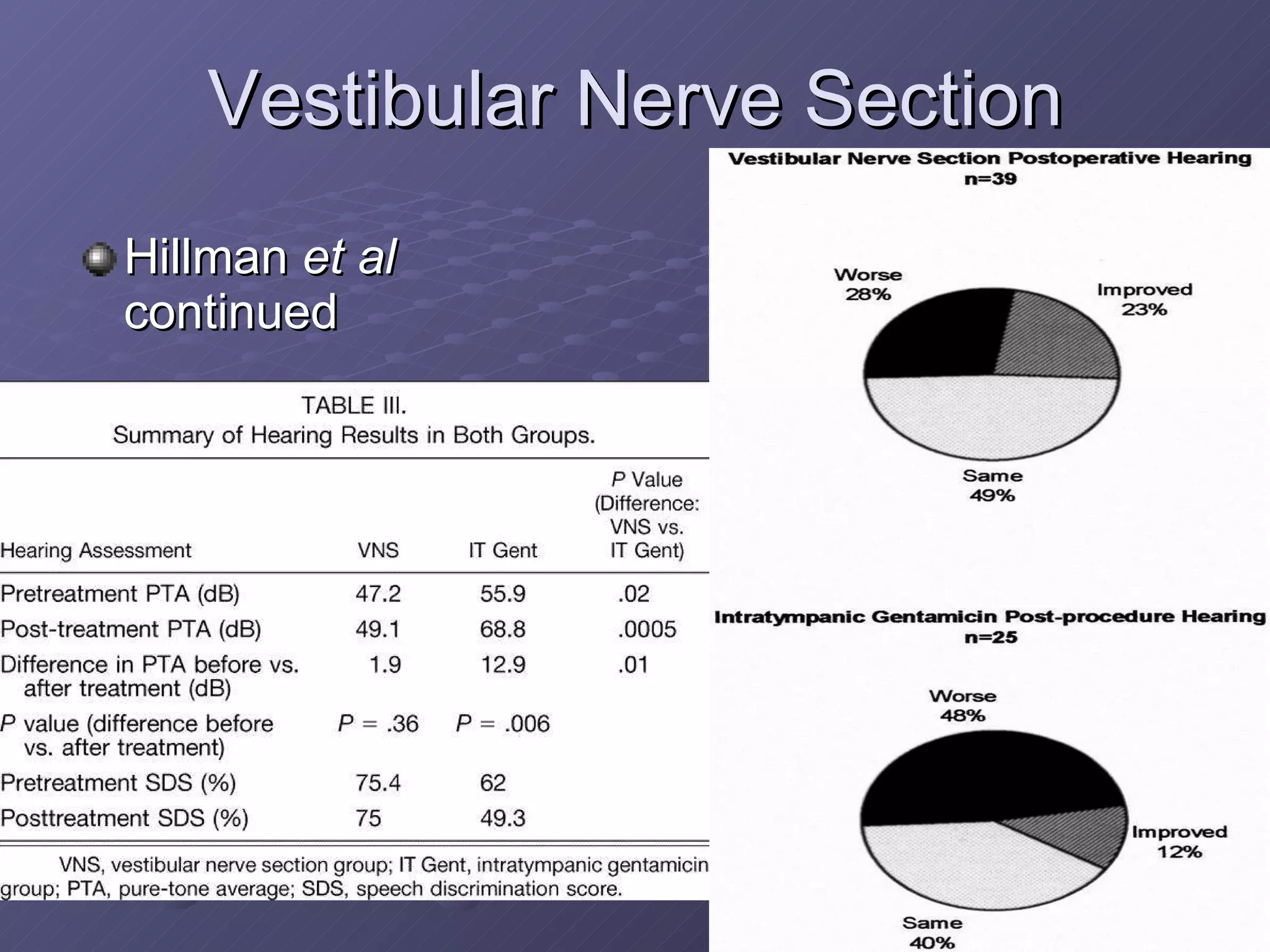



The document discusses various treatment controversies for Meniere's disease. It outlines the history and definition of the disease, as well as current understandings of physiology and pathophysiology. It then summarizes different medical, mechanical, intratympanic, surgical, and ablative treatment options and discusses evidence from studies evaluating their efficacy and side effects, finding that many options remain unproven or controversial while intratympanic gentamicin titration and vestibular nerve section/labyrinthectomy can reliably reduce vertigo.























































































