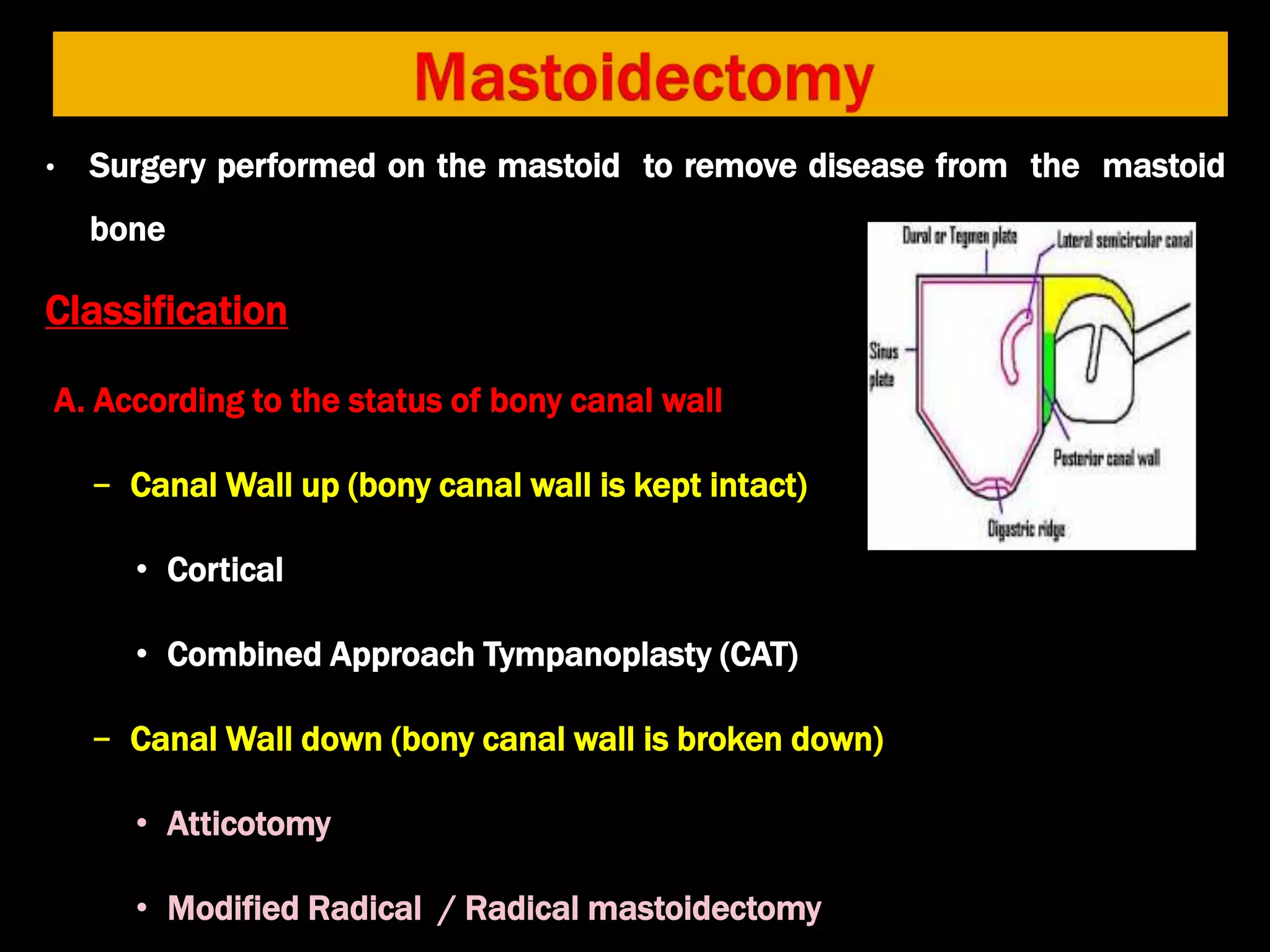
The document outlines various mastoid surgeries aimed at removing disease from the mastoid bone, classified by the status of the bony canal wall and the extent of tissue removal. It discusses the objectives of these surgeries, such as eradicating infections, preserving hearing, and ensuring a satisfactory cosmetic outcome, while also detailing the surgical approaches, advantages, and disadvantages. Additionally, it highlights potential complications and the importance of thorough disease removal to avoid recurrence.






























































![Untitled (6) [Autosaved] ear.pptx ear surgeries](https://cdn.slidesharecdn.com/ss_thumbnails/untitled6autosavedear-251128030434-d7ae6d96-thumbnail.jpg?width=640&height=640&fit=bounds)














































