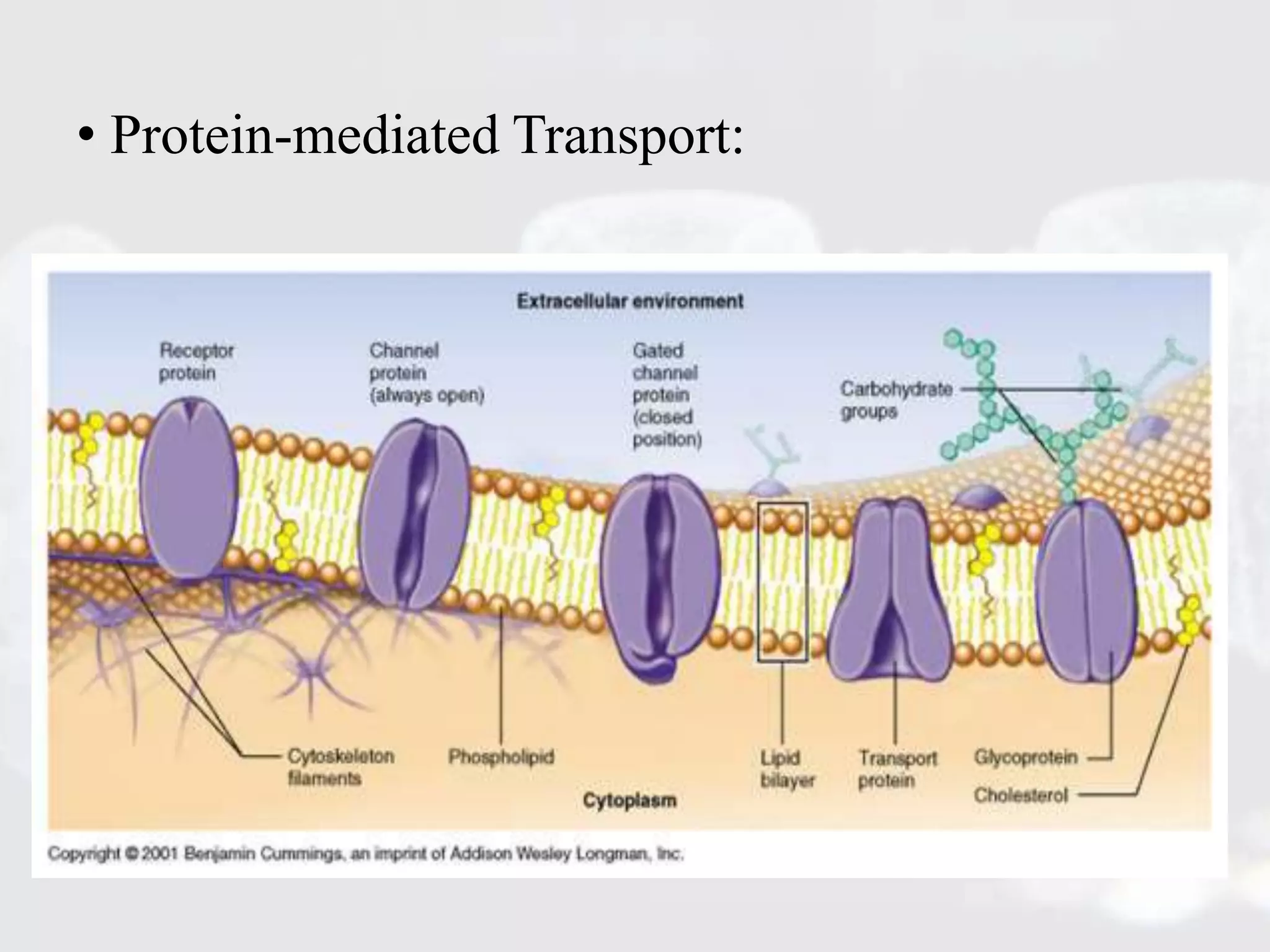
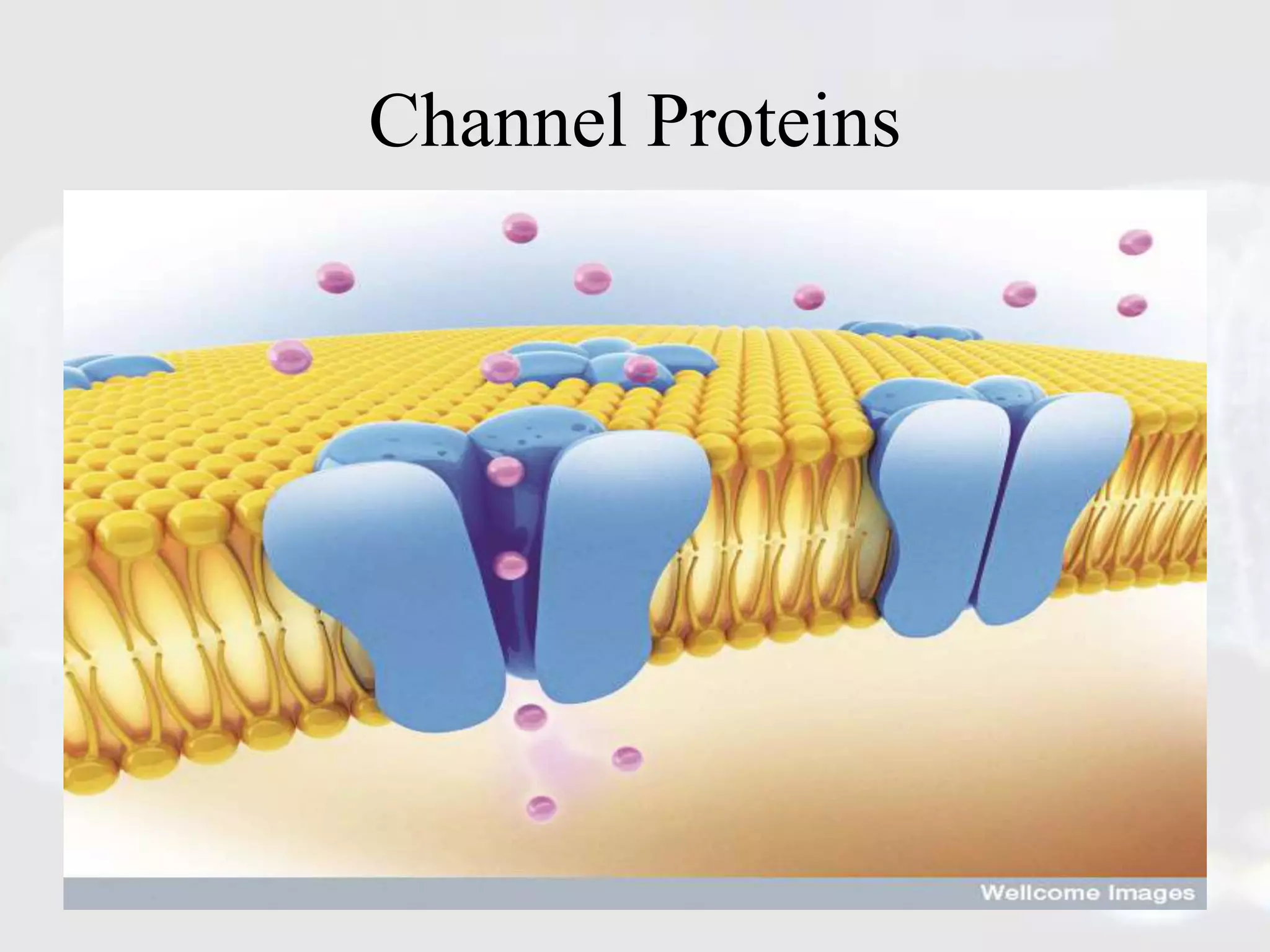
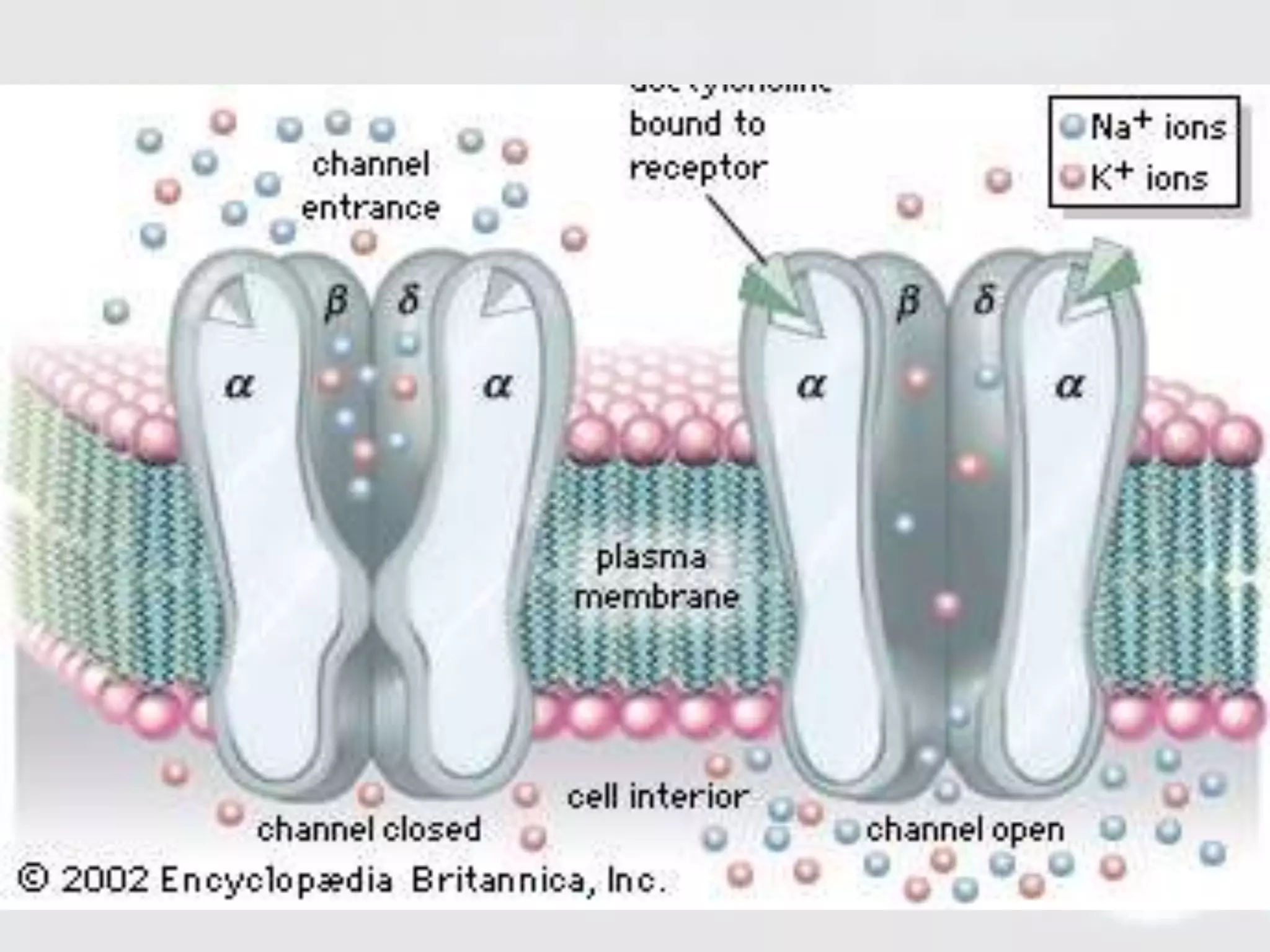
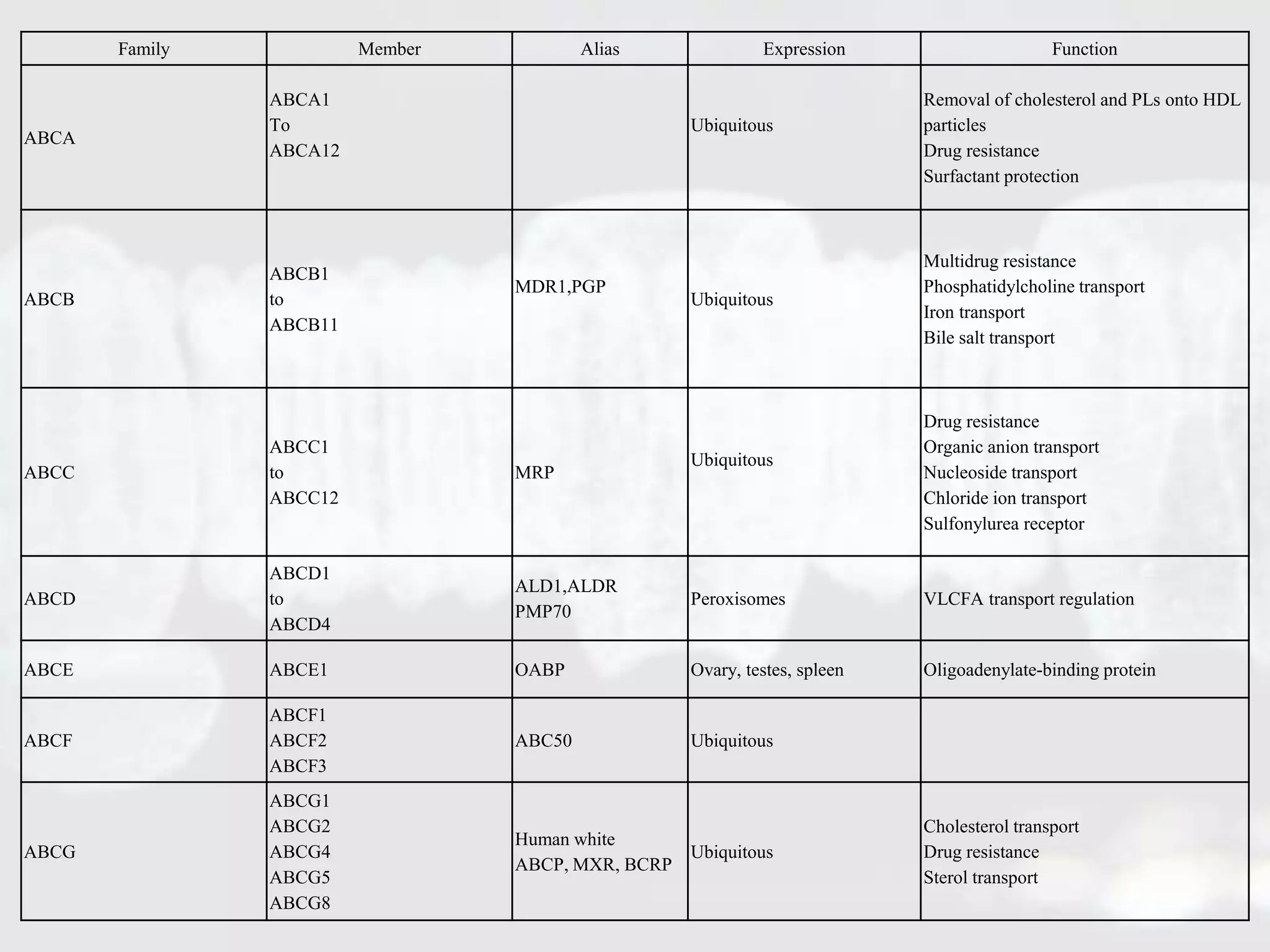
Membrane transporters play an important role in drug absorption, distribution, and elimination. There are two main types of membrane transport proteins - channels and carriers. Channels passively transport ions and molecules via protein-lined pores, while carriers actively transport substances against concentration gradients using energy from ATP or ion gradients. Important carrier families include ABC transporters like P-gp and MRP, which pump various drugs and toxins out of cells, and SLC transporters like OATP, OCT, and MATE, which transport organic ions and molecules into and out of cells. Variations in membrane transporters can significantly impact drug pharmacokinetics, pharmacodynamics, and adverse drug responses. Further research is still needed to fully understand