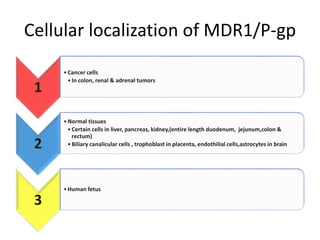
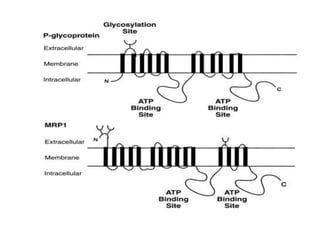
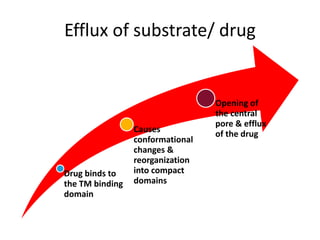
P glycoprotein is an efflux transporter that pumps certain drugs and toxins out of cells. It is expressed in the liver, kidneys, intestines and blood brain barrier, protecting tissues from harmful substances. P glycoprotein is a 170 kDa membrane protein composed of two symmetrical halves that contain transmembrane and ATP binding domains. It transports substrates by undergoing conformational changes upon ATP hydrolysis. P glycoprotein contributes to multi-drug resistance in cancer and limits oral absorption and brain penetration of many drugs. Genetic polymorphisms and drug interactions involving P glycoprotein inhibition or induction can significantly impact a drug's pharmacokinetics and toxicity.



































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








