This document discusses drug transporters and their role in drug absorption, distribution, metabolism and excretion. It covers the main types of transporters including ABC transporters like P-glycoprotein and SLC transporters. It describes how transporters regulate the movement of drugs across membranes in organs like the intestine, liver and kidneys. It also discusses how overexpression of transporters like P-glycoprotein can lead to multidrug resistance and the various approaches used to overcome resistance, such as inhibitors of transporter activity.
Introduction to drug transporters, types of transport, and their roles including ABC Superfamily.
Examples of transport phenomena and types; focuses on aquaporins and their function in water transport.
Examples of transport phenomena and types; focuses on aquaporins and their function in water transport.
Role of transporters in nutrient influx, waste efflux, and regulation of drug distribution and bioavailability.
Role of transporters in nutrient influx, waste efflux, and regulation of drug distribution and bioavailability.
Overview of ABC and SLC transporter families, their characteristics, and directional transport functions.
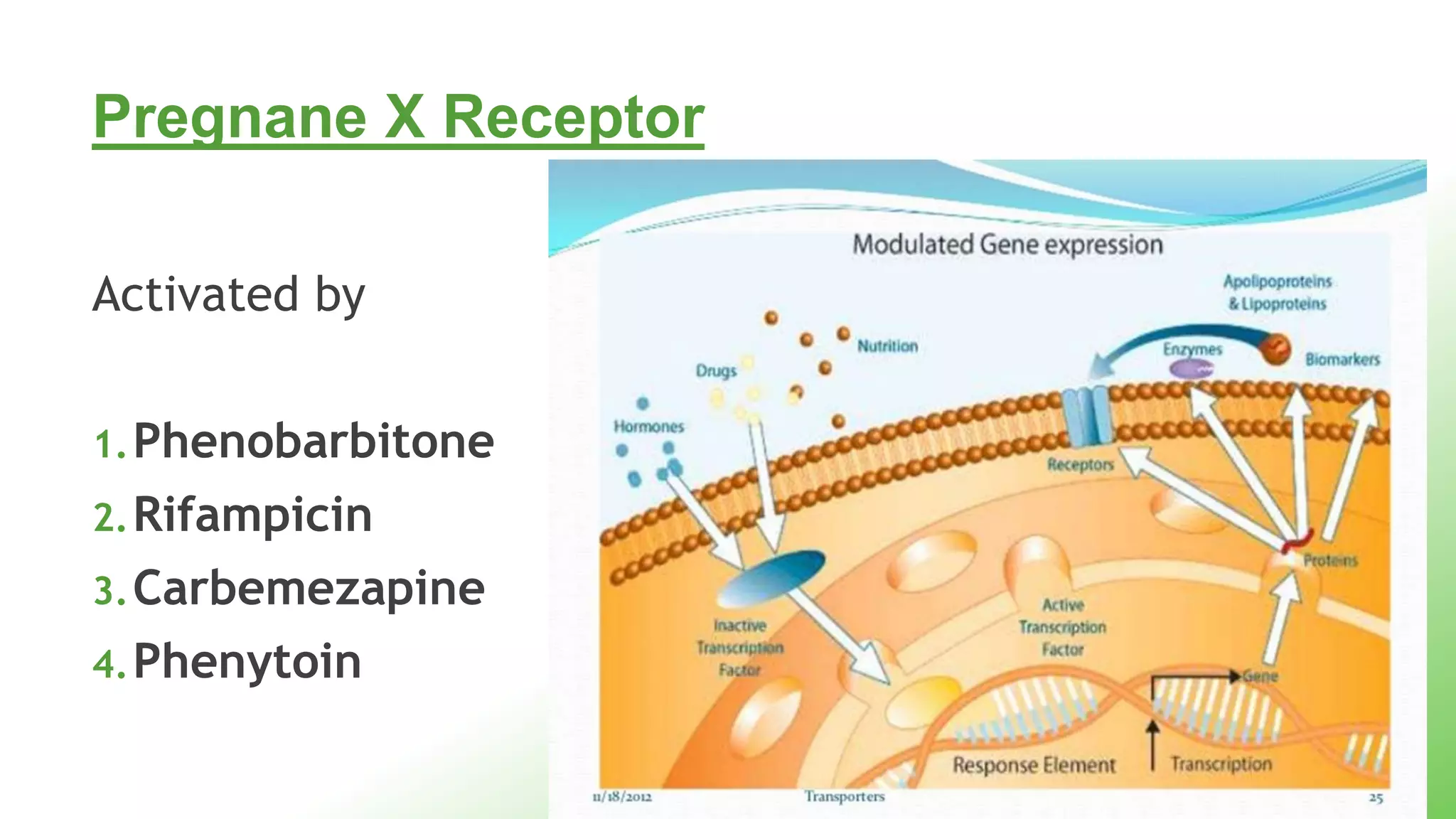
Regulatory mechanisms influencing transporter expression, including various receptor interactions.
Regulatory mechanisms influencing transporter expression, including various receptor interactions.
Structure and function of ABC transporters, their roles as importers and exporters, and their gene family classification.
Associations between ABC transporter families and genetic disorders like cystic fibrosis and others.
Details on SLC transporters, their classifications, and functional role in drug absorption in the intestine.
Details on SLC transporters, their classifications, and functional role in drug absorption in the intestine.
Interactions of specific drugs with transporters, focusing on hepatic and renal transporters and their clinical implications.
Interactions of specific drugs with transporters, focusing on hepatic and renal transporters and their clinical implications.
Function of organic anion transporters in drug reuptake and examples of endogenous and exogenous substances.
The role of transporters like P-glycoprotein in the development of drug resistance and its implications.
The role of transporters like P-glycoprotein in the development of drug resistance and its implications.
Functions, substrates, inhibitors, and the role of P-glycoprotein in drug resistance and clinical challenges.
Functions, substrates, inhibitors, and the role of P-glycoprotein in drug resistance and clinical challenges.
Strategies to combat multidrug resistance, including various generations of reversal agents and alternative approaches.Significance of transporters in regulating bioavailability, drug targeting, detoxification, and overcoming resistance.
Introduction
Typesof transport
Role of transporters
Regulation of transporters on genetic level
ABC Superfamily
P glycoprotein
SLC transporters
OAT/OCT
Hepatic transporters
Renal transporters
3.
A pt comesto you with chief
complaints of diarrhoea. He is
a known case of arrhythmias
on quinidine. You advice him
to take loperamide.
After taking the drug , he goes
into respiratory depression.
What do you think
happened?
Aquaporins
bi-directional membranechannels -transport
water
not ion channels- H2O is transported as an
uncharged molecule
driving force-osmotic gradient
13 AQP genes in the human genome
9.
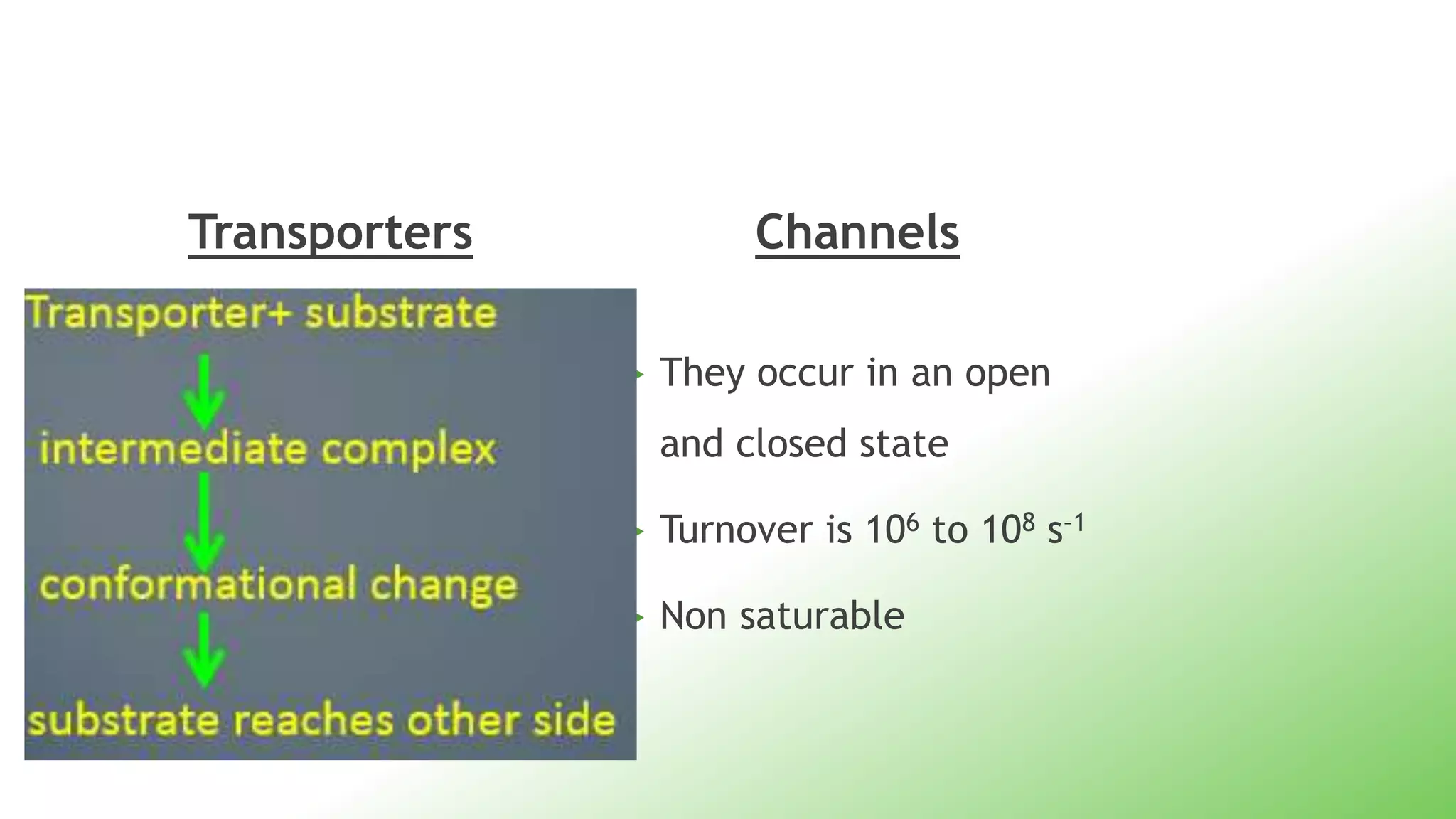
Transporters
It formsan intermediate
state with the substrate
Turnover is 101 to 103 s–
saturable
Channels
They occur in an open
and closed state
Turnover is 106 to 108 s–1
Non saturable
11.
Transporters
• membrane proteins
•control influx of essential nutrients and ions
• efflux of cellular waste, environmental toxins,
drugs, and other xenobiotics
• coded by 7% of the total number of genes
13.
Physiological Role ofTransporters
Regulates the distribution and bioavailability of
drugs
Removal of toxic metabolites and xenobiotics
from cells into urine,bile and intestinal lumen
Transport of compounds out of the brain across
the blood brain barrier
15.
Types of membrane
transporters
2000 genes in humans code for transporters or
transporter related proteins
2 major superamilies- ABC and SLC
Most ABC proteins are primary active transporters
SLC superfamily includes facilitated transporters and
ion coupled secondary active transporters
16.
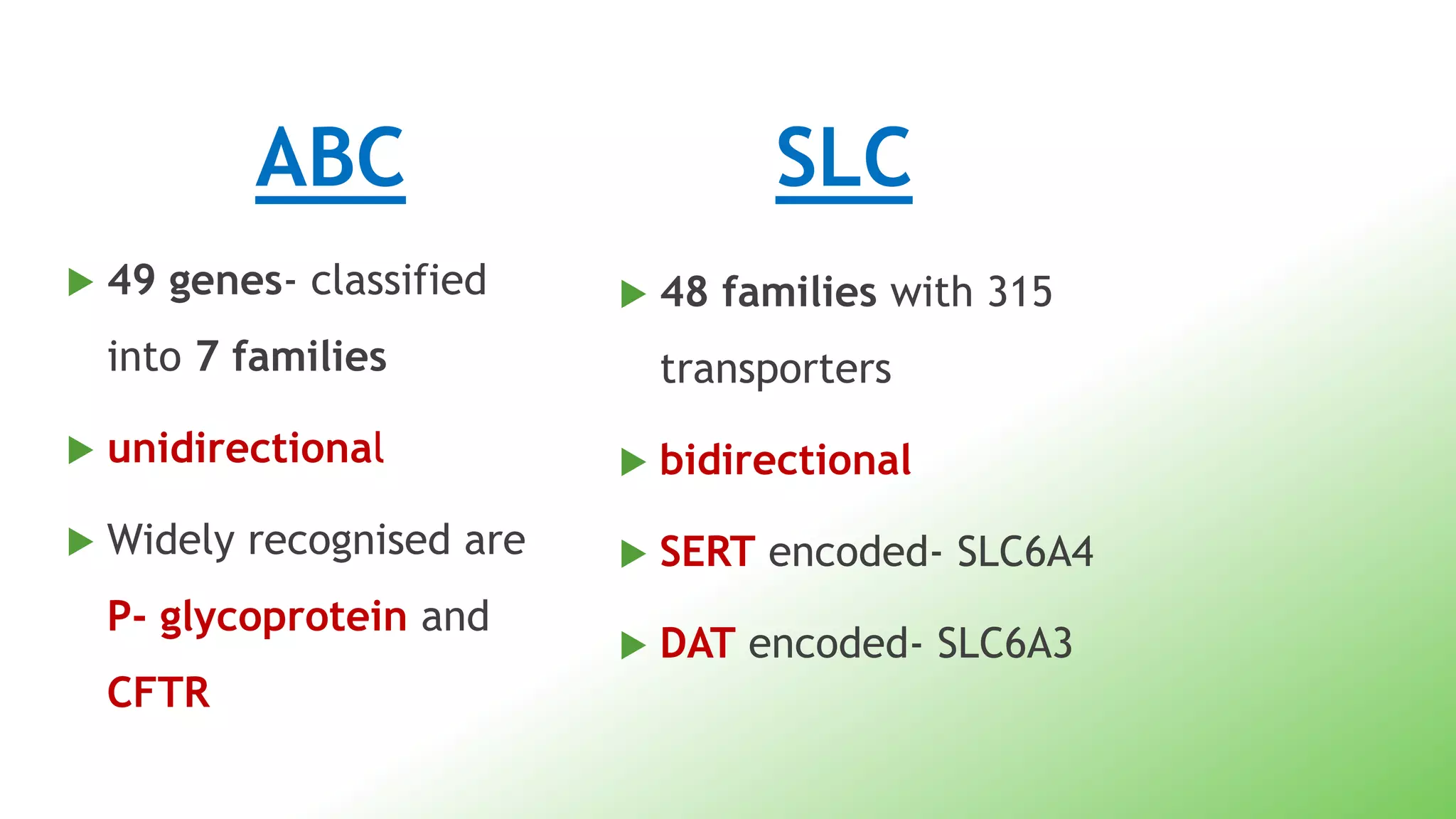
ABC
49 genes-classified
into 7 families
unidirectional
Widely recognised are
P- glycoprotein and
CFTR
SLC
48 families with 315
transporters
bidirectional
SERT encoded- SLC6A4
DAT encoded- SLC6A3
What does theterm ‘vectorial’
imply??
Transport of an ion or molecule across an
epithelium in a certain direction (e.g.
absorption of glucose by the gut).
Vectorial transport implies a nonuniform
distribution of transport proteins on the plasma
membranes of two faces of the epithelium.
ATP Binding CassetteTransporter
protein superfamily
Transmembrane proteins
utilize the energy of ATP hydrolysis
48 ABC genes in humans
Can be divided into 7 groups
Structure
The commonstructure of all ABC – consists of 2
Distinct domains
Transmembrane domain (TMD)
Nucleotide binding Domain (NBD)
29.
In mostExporters- the N terminal TMD and C terminal
NBD are fused to form a single polypeptide chain
arranged as TMD-NBD-TMD-NBD
Importers- have an inverted organisation- NBD-TMD-
NBD-TMD where the ABC domain is N- terminal
whereas the TMD is C terminal
GENE
NAME
FAMILY
NAME
NO. OF
FAMILIES
DIS. ASOCIATED
ABCAABC A 12 • Tangiers dis
• Stargadts dis
ABCB ABC B 11 • PFIHC
ABCC ABC C 13 • Cystic fibrosis
• Dubin Johnson syn
ABCD ABC D 4 • Adreno-leukodystrophy
ABCE ABC E 1
ABCF ABC F 3
ABCG ABC G 5 • Sitosterolemia
SLC Transporters
Includes48 families and represents 315 genes in
human genome
Contain hydrophobic transmembrane alpha
helices
Includes facilitative transporters and secondary
active transporters
Various transportersare expressed on the brush
border of the intestine
Influx transporters expressed In the gut,
improve absorption eg. PEPT-1, OATB1
PEPT1- mediates transport of drugs-
B-Lactams, ACEI, Valacyclovir
Efflux transporters limit the absorption of drugs
eg. P gp, BCRP, MRP2
47.
BCRP
member ofthe ABC Transporter family
Plays role in secretion of topotecan
When topotecan, substrate for BCRP and
GF120918( ELACRIDAR), an inhibitor of both
BCRP and P gp were administered orally,
bioavailability of topotecan was increases in P-
gp deficient mice
48.
• BCRP Isexpressed also in the
bile canalicular membrane
and placenta
• In pregnant GF120918
Treated P gp deficient
mice,fetal penetration of
topotecan was 2 fold higher
49.
Oral drug inhibitortransporter
Digoxin quinidine P gp
Paclitaxel Cyclosporin P gp
methotrexate Omeprazole BCRP
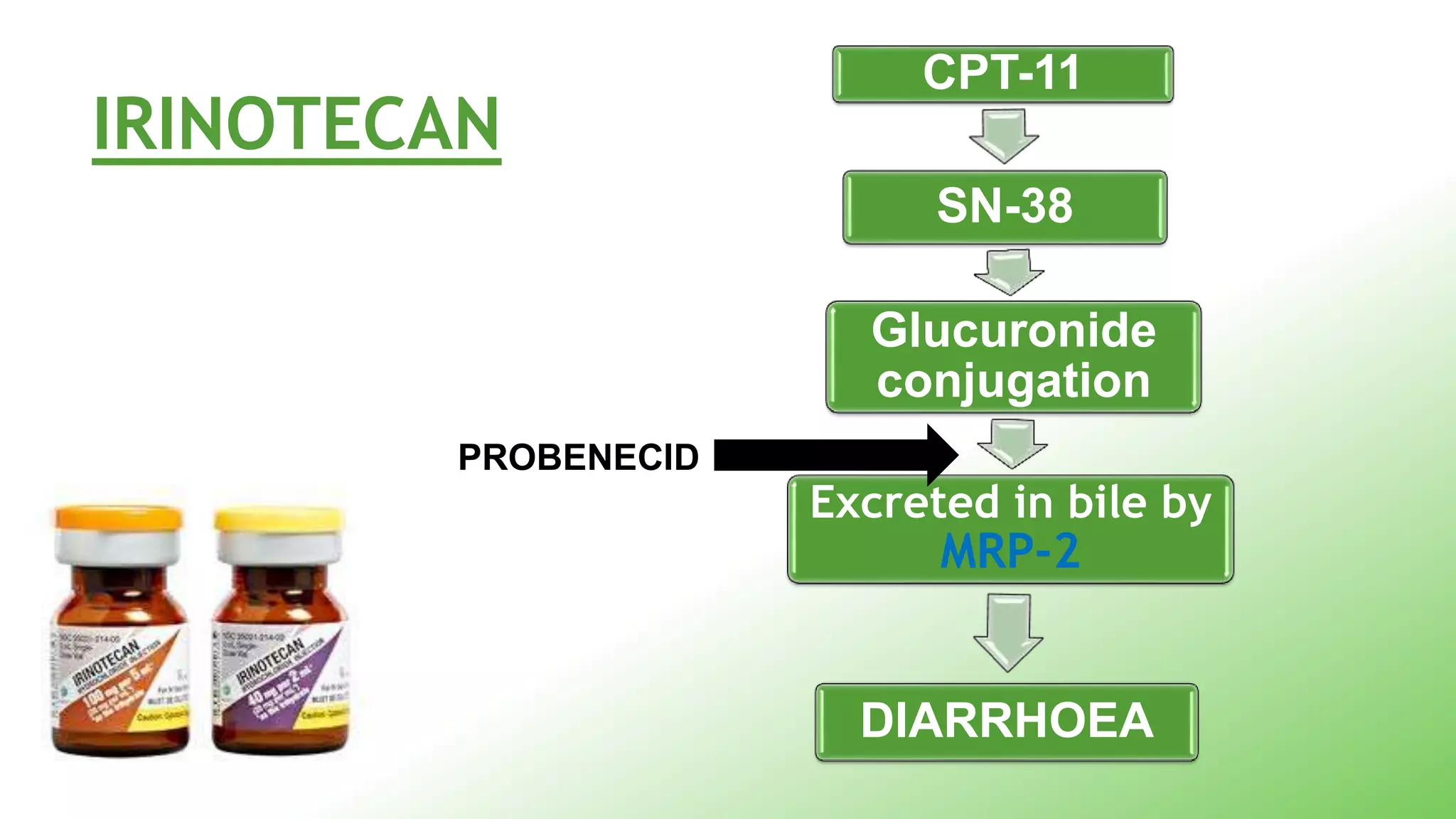
irinotecan gefitinib BCRP
Temocapril
Temocaprilat- excretedin both bile and urine
Plasma concentration of temocaprilat remains
unchanged even in patients of renal failure
Temacoprilat is a bisubstrate of OATP and MRP2,
whereas other ACEI are not good substrates of
MRP2
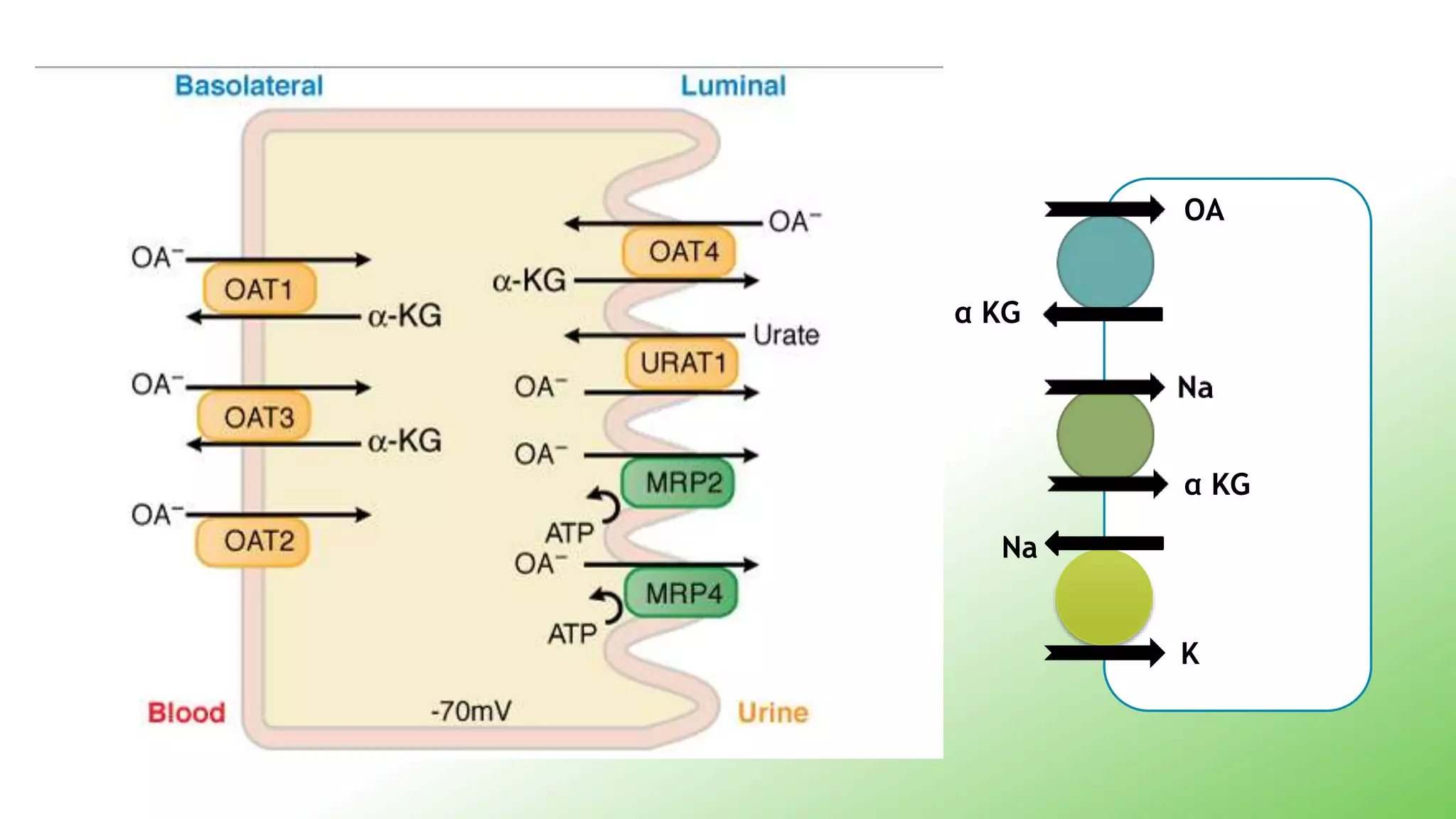
Renal Transporters
Renaltransporters play an
important role in drug
elimination ,toxicity and
response
Transporters may have dual
specificity for organic anions
and cations
Role in CNS
Involved in neuronal reuptake- SLC1 and
SLC6
SLC6 responsible for reuptake of
1. norepinephrine
2. dopamine
3. serotonin
4. GABA
65.
SLC6A1 /GAT1-Target for the drug tigabine
SLC6A2/NET - Target for despramine
SLC6A3/DAT- cocaine and its analogs
SLC6A4/SERT- Target for fluoxetine and
paroxetine
In 1976, Lingreported
the overexpression of a
membrane protein in
colchicine resistance
Chinese hamster ovary
cells, acquired
resistance to various
other drugs!!
68.
Q.1. What isthe genetic
basis???
Q.2. How frequency will it
occur?????
• 170 kDatransmembrane glycoprotein
• ATP-dependent drug efflux pump
• responsible for decreased drug accumulation
• mediates the development of resistance to
anticancer drugs
• also functions as a transporter in the BBB
72.
P gp inhumans
MDR1
Responsible for
efflux of drugs
MDR2
Transport of
phosphatidylcholine
to bile
Relation between Pgpand
cyp3A4
Both are regulated by PXR
P gp keeps intracellular concentration
within the range of CYP3A4
Metabolism results In better substrates of
P gp
cyp3A4
P gp
Transporters and drugresistance
Play a critical role in developing resistance to
Anti cancer
Anti microbials
Anti epileptics
85.
Why resistance isso important to
study?
result in treatment failure
increased costs,
prolonged duration of hospital stay
higher morbidity and mortality rates
Approaches to overcomeMDR
1. REVERSAL AGENTS
known as chemosensitisers
inhibit P gp
increase intracellular concentration of the drug
89.
First generation agents
Have their own pharmacological action
Were used in high doses
Not selective to P gp
Therefore, high toxicity
1. Cyclosprine – hepatic, renal, myeloid ,
neurotoxicity
2. Verapamil- cardiotoxicity
90.
Second Generation Agents
Selective and less toxic
Substrates of P gp and CYP3A4
Lead to unpredictable absorption and
metabolism
1. Valspodar ( R enantiomer of verapamil)
2. Biricodar
91.
Third generation agents
Agents were not substrates of CYP3A4
Selectively and potentially inhibit Pgp
1. Tariquidar XR9576
2. Zosuquidar LY335979
3. Laniquidar R101933
93.
Newer ways toovercome MDR
Monoclonal Ab- MRK 16- reversed MDR in
transgenic mice
Epothilones- not recognised by P gp
Increase rate of influx of anticancer drug
by increasing lipophilicity of the compound
94.
So why dowe need these
transporters???
To regulate bioavailability
To act as drug targets
To eliminate toxins
To overcome resistance
95.
Involvement of atransporters is
more of a rule than an
exception!!!!
#29 The TMD also known as Membrane Spanning Domain (MSD) OR Integral Domain (ID) consists of alpha helices embedded in lipid bilayer
It recognises substrates and undergoes conformational change
The sequence and architecture of TMD is variable, reflecting the chemical diversity of substrates that can be translocated
The NBD is located in the cytoplasm
Site for ATP binding
#31 Exporters have an Intracellular domain (ICD) that joins the membrane spanning helices and ABC domain
The ICD is believed to be responsible for communication between TMD and NBD
#32 This model presents 2 principal conformation of the NBDs
Formation of a A closed dimer on binding of the 2 ATP molecules
Dissociation to an open dimer facilitated by the ATP hydrolysis
Switching between the 2 conformations induces a conformational change in the TMD resulting in substrate translocation
#33 Importers have a High Affinity Binding protein that specifically associates with the substrate in the periplasm
The substrate binding site alternates between Outward and Inward facing conformation
The relative binding affinities of the two conformations of the substrates determines the net direction of transport
For importers- outward facing conformations have a higher binding affinity for the substrate
Exporters - inward facing conformations have a higher binding affinity for the substrate
#45 PEPT-SLC15 Cefaplexin and not cefazolin
P gp affects the absorption of many drugs because of its broad substrate specificity
Intestinal P gp content correlates with the AUC after oral absorption of drugs like digoxin
Eg. patient undergoing a small bowel transplant demonstrated that the plasma level of tacrolimus-a substrate for for both cyp 3A4 and P gp correlated more with the levels of P gp
#48 Abcg2- It has only 1 ATP binding cassette- half transporter
#53 NTCP-
Hepatic uptake of anions, cations, bile salts is mediated by SLC Transporters in the basolateral membrane of hepatocytes
OAT-transport of anions
OCT and NCTP –transport cations and bile salts
ABC Transporters like BSEP, MDR1, MRP2 In the bile canalicular membrane of hepatocytes mediates the efflux of drugs from liver to bile
Ntcp-sodium taurocholate co trnsporter
Imhibition of BSEP thru drugs lik troglitazone and rifampicin may lead to cholestasis
#55 They together help In minimising the escape of these drugs into systemic circulation
#56 Drugs that are excreted in both bile and urine to the same degree and thus are expected to have minimal interindividual variations in their pharmacokinetics
#57 potent anticancer drug
late-onset gastrointestinal toxic effects, such as severe diarrhoea
#58 Secretion in the kidney is ritical in the body’s efence mechanisms against foreign substances
#61 For the transepithelial flux of a compound, the compounds traverse 2 membranes
OCT are Involved in the uptake of cations into liver or kidney from blood
OCT1 and OCT2- epithelial cells of kidney, liver and intestines
Located in the basolateral membrane
Organic cations cross the basolateral membrane by 3 distinct transporters in the SLC family
OCT1- SLC22A1
OCT2- SLC22A2
OCT3- SLC22A3
They are transported across this membrane down their electrochemical gradient
Transport across the apical membrane occurs via proton organic cation exchange mechanism
Transporters in the apical sde- novel org cations
They r bifunctional..in d reuptake mode,they functn as sodium cotransporters relyng on inwardly driven Na gradient to move carnitine
MATE-SLC47
#63 Two primary transporters on basolateral membrane
OAT1 (SLC22A6)
OAT3 (SLC22A8
#66 SLC6A/GAT1- most important GABA Transporter-presynaptic neurons
antidepressant desipramine -selective inhibitor of NET
In ADHD- methyphenidate-inhibits NET
SLC6A11/GAT3- Target of anticonvulsants
#82 In the case of fast absorbing drugs having larger doses, efflux by P-gp poses less impact on drug absorption
the transport activity of P-gp becomes saturated by high concentrations of drug in the intestinal lumen.
the case of drugs requiring a very small dose for their pharmacological actions or the drugs that have very slow dissolution and diffusion rates, P-gp mediated drug efflux greatly interferes with their delivery. As it decreases drug absorption, those small amounts of drugs cannot reach the blood circulation in sufficient quantity and, at times, can be life threatening. sustained release dosage forms of the substrates-ineffective
#85 P gp is overexpressed in cancer cells
Other transporters implicated in drug resistance are
BCRP ( Breast Cancer Resistance protein)
OAT (Organic Anion Transporter)
MRP ( Multidrug reistance protein)
Overexpression of MRP4 – Resistance to antiviral nucleoside analogues
#86 Drug efflux-reduce intracellular drug concentrations
#93 Natural polymers
Anionic gums : xanthan gum- P gp inhibitor at 0.05%
From green tea- polyphenols
From grapefruit juice- various polysaccharides like D- glucose
thiomers- form disulphide bond between cysteine
group of P gp and free thiol group of
thiomer
eg. α- chitosan-thiobutylamidine
Liposomes
They are vesicles made of bilayer- contain phospholipid and hydrophilic aqueous region
Drug is encapsulated in this carrier
Neutral PL are selectively pumped out- so competition for P-gp