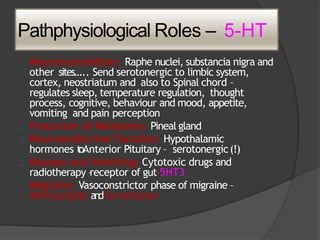
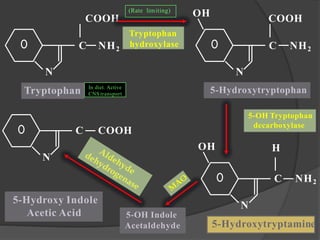
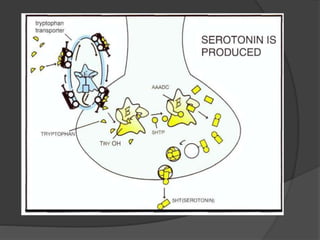
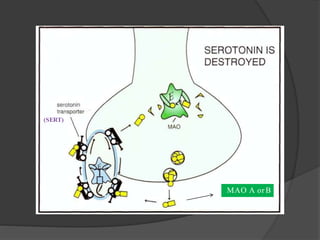
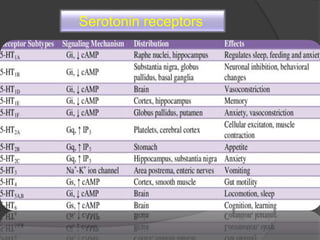
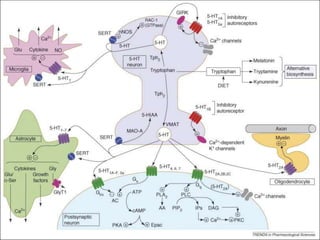
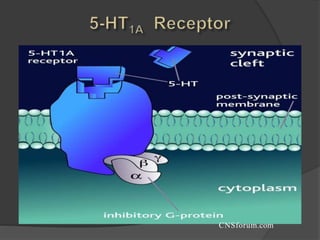
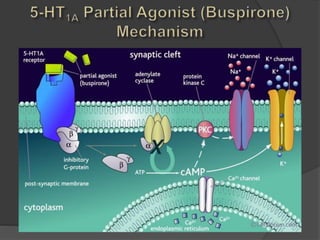
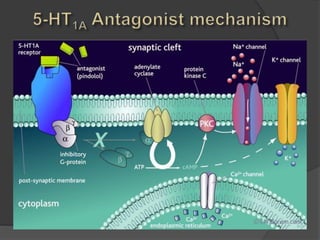
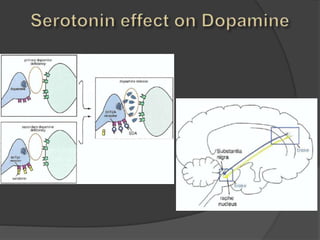
Serotonin is a monoamine neurotransmitter synthesized from tryptophan. It is found extensively in the gastrointestinal tract and in serotonergic neurons in the central nervous system. Serotonin receptors include 5-HT1-7 and are involved in various physiological functions like mood, appetite, sleep, and pain perception. Imbalances in the serotonergic system are associated with disorders like depression, anxiety, schizophrenia, and impulse control disorders. Drugs that affect the serotonergic system include SSRIs, SNRIs, triptans, 5-HT3 antagonists, buspirone, and MAOIs.





















![Serotonin Pharmacology (5-HT) [Neurotransmitter]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085115-thumbnail.jpg?width=640&height=640&fit=bounds)







































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















