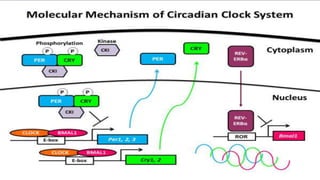
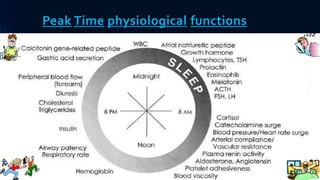
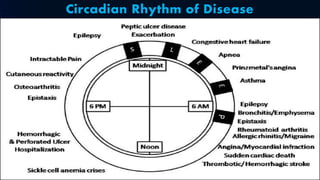
The document discusses the principles of circadian rhythms and chronobiology, emphasizing the importance of timing in pharmacotherapy to optimize drug efficacy and minimize side effects. It details various biological rhythms that influence medication absorption, metabolism, and elimination, along with specific examples across different drug classes. The conclusion suggests the need for ongoing research into chronophramacology to enhance treatment outcomes by aligning drug delivery with the body's biological clock.