DRUG DISPOSITION :
Drug disposition is a general term that encompasses the four processes
that determine drug and metabolite concentrations in plasma, in tissue,
and within cells: absorption, distribution, metabolism, and excretion
(usually biliary or renal).
3.
DRUG TRANSPORTATION ACROSSTHE CELL
MEMBRANE :
The movement of drug from one side of biological barrier to the other is called Bio-
transport and the mechanism underlying the transfer of drug across biological
barriers are called the transport mechanism.
The major transport mechanisms are :
1. Passive Diffusion
2. Carrier mediated Transport
a. Active Transport
b. Carrier mediated Diffusion
3. Pinocytosis or Phagocytosis
ACTIVE TRANSPORT
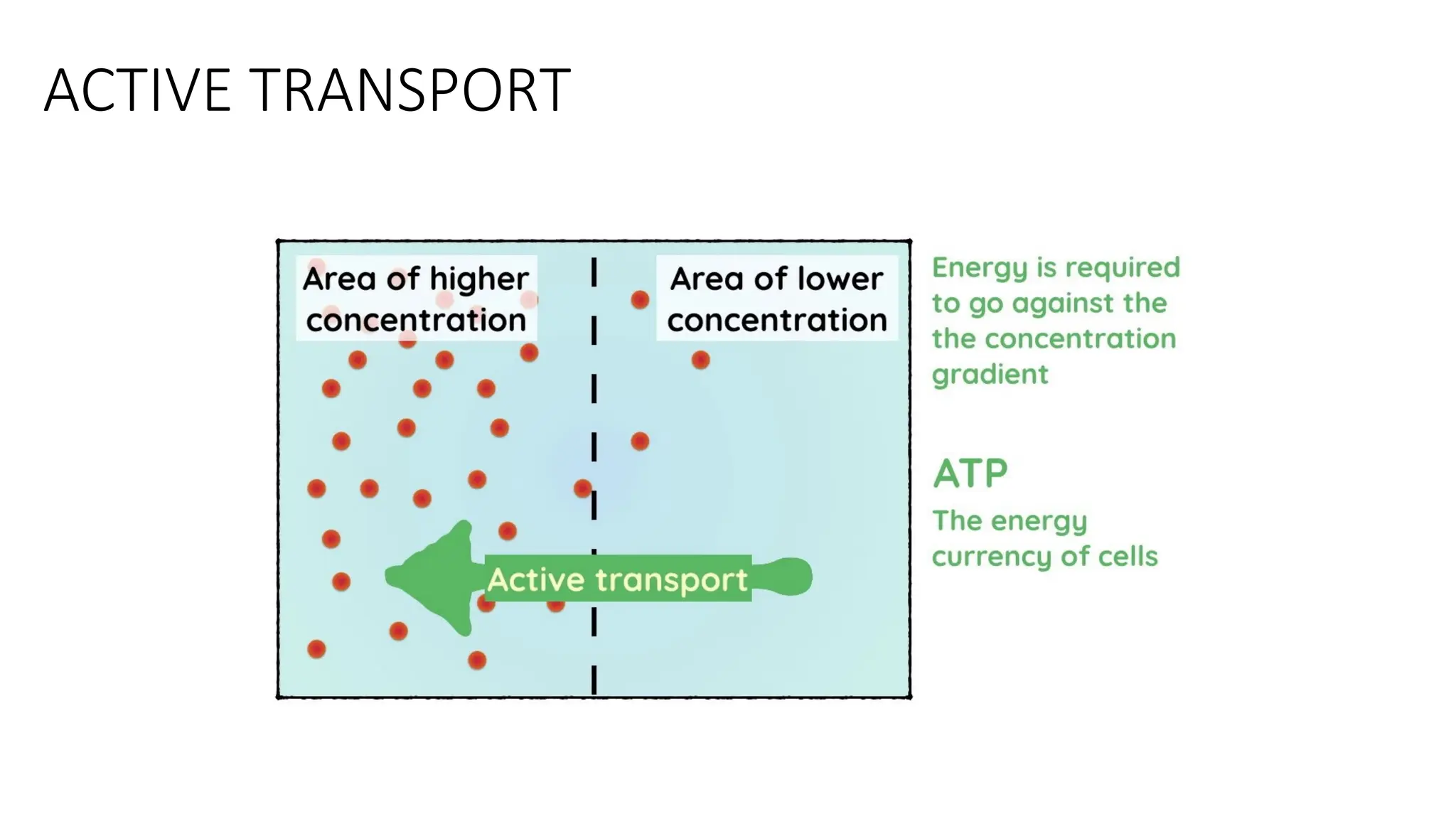
Incellular biology, active transport is the movement of molecules across a membrane
from a region of their lower concentration to a region of their higher concentration—
against the concentration gradient.
Active transport requires cellular energy to achieve this movement.
There are two types of active transport:
Primary active transport
Secondary active transport
Ex. : An example of active transport in human physiology is the uptake of glucose in
the intestines.
6.
ACTIVE TRANSPORT
Activetransport is usually associated with accumulating high concentrations of
molecules that the cell needs, such as ions, glucose and amino acids.
If the process uses chemical energy, such as from adenosine triphosphate (ATP), it is
termed Primary active transport.
Secondary active transport involves the use of an electrochemical gradient.
PRIMARY TRANSPORT MECHANISM:
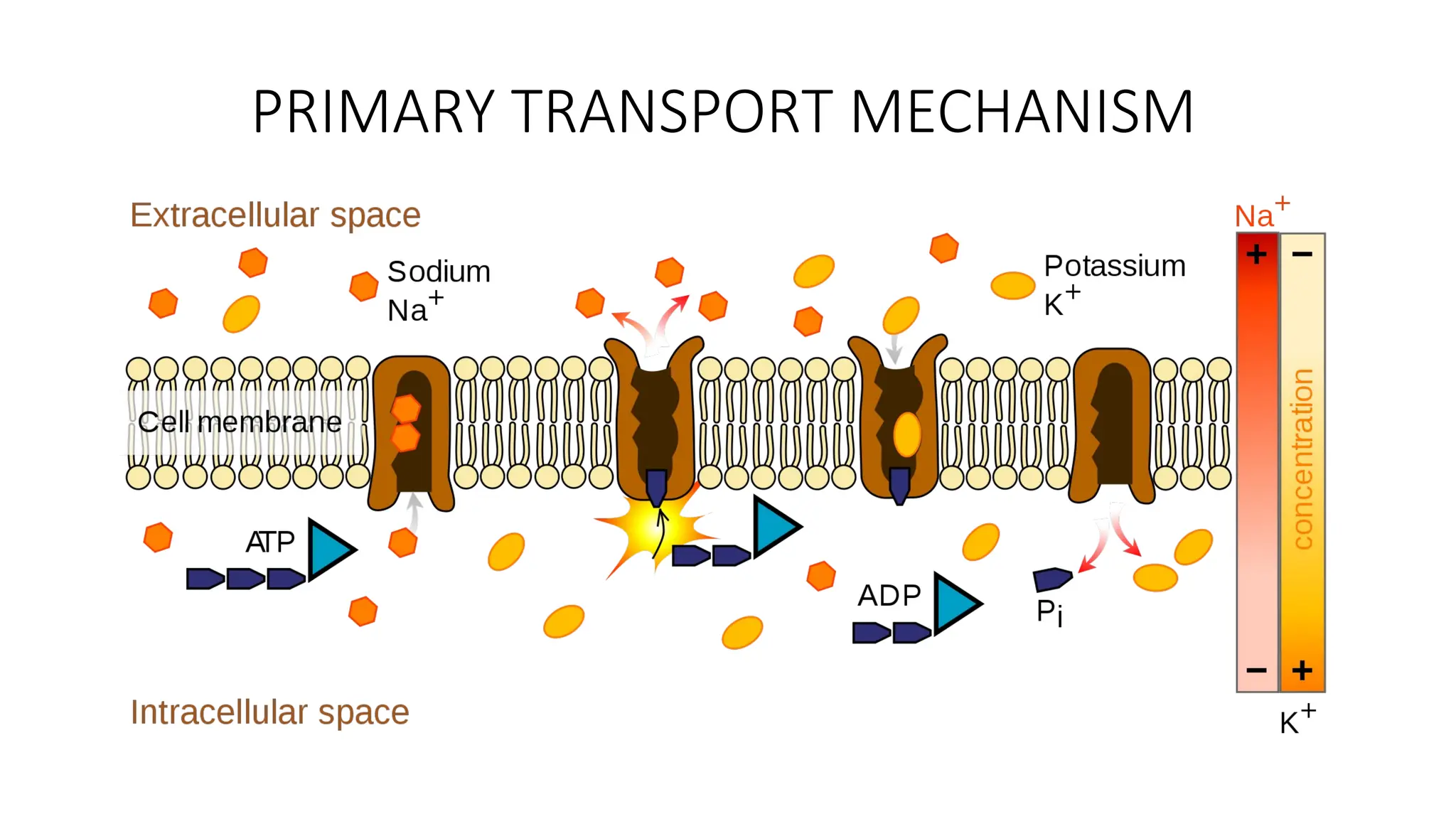
•One of the most important pumps in animal cells is the sodium-
potassium pump, which moves Na+
out of cells, and K+
into them.
Because the transport process uses ATP as an energy source, it is
considered an example of primary active transport.
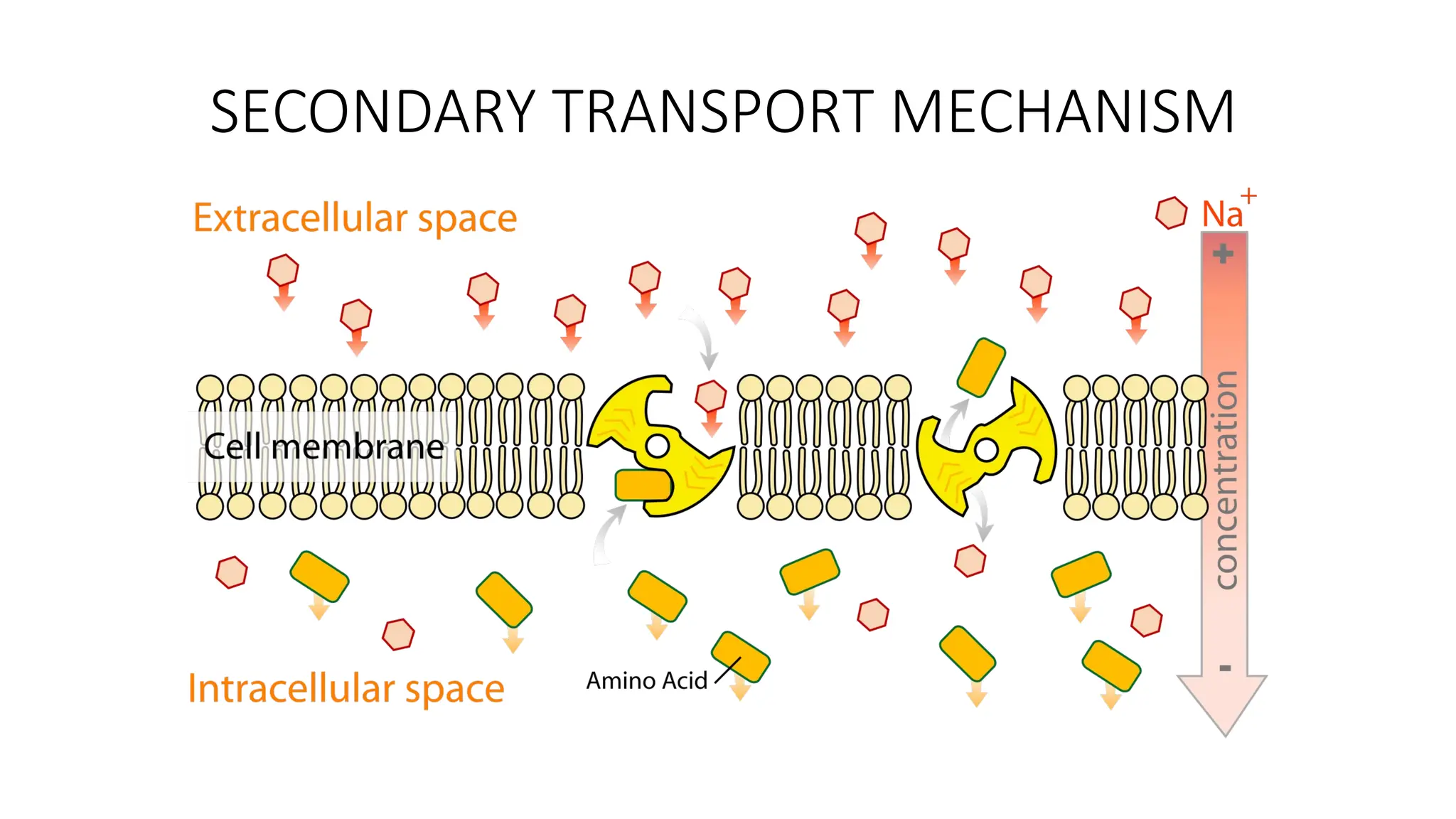
SECONDARY TRANSPORT MECHANISM:
•The electrochemical gradients set up by primary active transport
store energy, which can be released as the ions move back down
their gradients. Secondary active transport uses the energy stored in
these gradients to move other substances against their own
gradients
12.
MEMBRANE TRANSPORTERS :
•They are specialized proteins embedded in the cell membrane
that helps to movement substance like ions, nutrients, drugs, etc.
in and out of cell, that control influx and efflux of essential
nutrients and ions, and the efflux of cellular waste,
environmental toxins, drugs and other xenobiotics .
• They exhibits selectivity, and competitive inhibition by co-
transported substances.
13.
TYPES OF MEMBRANETRANSPORTERS :
• ABC Transporters
• Solute Carrier Transporters
TRANSPORTER
S
TRANSPORTERS :
• Transportersshould be an integral part of any ADMET modeling program,
because of our limited understanding of transporters, most prediction
programs do not have a mechanism to incorporate the effect of active
transport.
• However, interest in these transporters has resulted in a relatively large
amount of in vitro data , which in turn have enabled the generation of
pharmacophore and QSAR models and many of them.
16.
TRANSPORTERS :
• Thesemodels helps in understanding of the complex effects of
transporters on drug disposition, including absorption, distribution, and
excretion. Their incorporation into current modeling programs gives
accurate prediction of drug disposition behaveour.
• In-Silico modelling of targets of drug delivery can be done.
17.
TRANSPORTERS :
Some ofthe Active transporters which can be modelled are
discussed as follows :
• P-GP
• BCRP
• NT
• HPEPT 1
P-GP [P-glycoprotein]
• P-glycoprotein(P-GP)is an ATP-dependent efflux transporter that transports a broad
range of substrates out of the cell. It affects drug disposition by reducing absorption
and enhancing renal and hepatic excretion.
• For example, P-GP is known to limit the intestinal absorption of the anticancer drug
Paclitaxel and restricts the CNS penetration of human immune deficiency
virus(HIV)protease inhibitors. It is also responsible for multidrug resistance in cancer
chemotherapy.
• Because of its significance in drug disposition and effective cancer treatment, P-GP
attracted numerous efforts and has become the most extensively studied transporter,
with abundant experimental data.
20.
Cellular localization ofP-GP :
• Adrenal gland shows high levels of p-GP, diffusely distributed on the surface of cells in
both the cortex and medulla.
• In kidney, p-GP is found concentrated on the apical surface of epithelial cells of the
proximal tubules.
• In pancreas, P-GP is found on the apical surface of the epithelial cells of small ducts
but not on larger pancreatic ducts.
• Both colon and jejunum show high levels of p-GP on the apical surface of superfiacial
columnar epithelial cells
21.
EFFLUX OF SUBSTRATE/DRUGTHROUGH CENTRAL PORE:
• P-GP intercepts lipophilic drugs as they move through the lipid membrane
and flips the drugs from inner leaflets to the outer leaflets and to extra
cellular medium.
• A major reorganization of the transmembrane domains occurs through
out the entire depth of the membrane resulting in central pore formation
of 2-3 nm diameter and 5-6 nm in depth on binding of ATP.
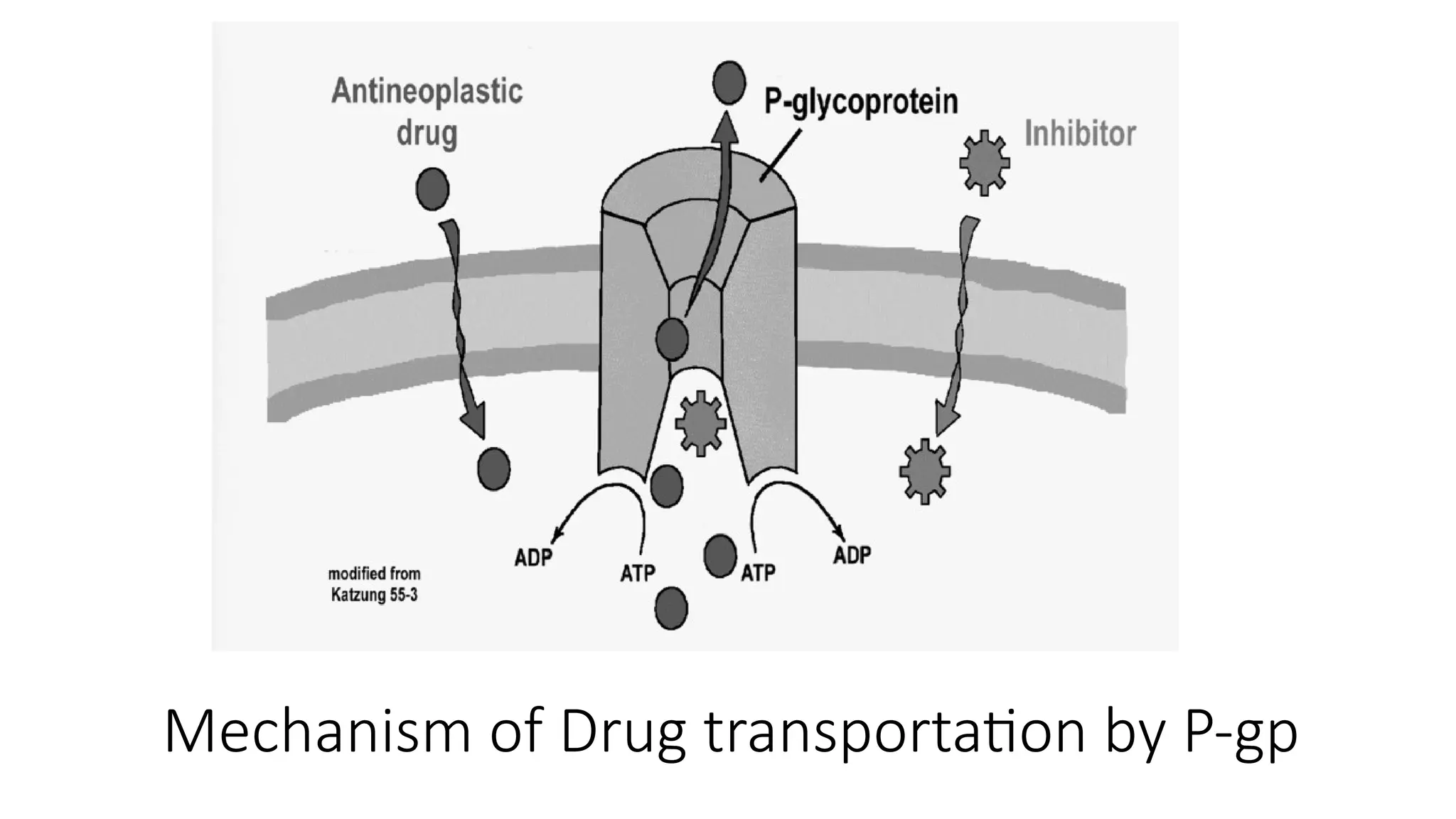
Mechanism of Drugtransportation by P-gp:
This slide shows how P-glycoprotein (P-gp) helps remove certain drugs from
the cell. P-gp is a special protein found in the cell membrane. When a drug,
like a cancer medicine (antineoplastic drug), enters the cell, P-gp can push it
back out. To do this, it uses energy from a molecule called ATP. This means
the drug doesn't stay in the cell long enough to work properly. Some
substances, called inhibitors, can block P-gp and stop it from removing the
drug. This helps the medicine stay inside the cell and be more effective.
This process is important because it explains why some medicines don’t
work well in certain cases, especially in cancer treatment.
24.
FUNCTIONS OF P-GP
•Drug Efflux: Pumps drugs out of cells, reducing their intracellular concentration.
• Protective Barrier: Found in the intestine, liver, kidney, and blood-brain barrier to protect the
body from harmful substances.
• Limits Drug Absorption: In the intestine, it decreases drug absorption by moving drugs back
into the gut.
• Enhances Drug Elimination: In the liver and kidneys, it helps remove drugs via bile and urine.
• Prevents Brain Exposure: At the blood-brain barrier, it blocks drugs from entering the brain.
• Multidrug Resistance (MDR): Overexpression in cancer cells leads to resistance by pumping
out anticancer drugs.
• Affects Drug Bioavailability: Influences how much of a drug reaches the bloodstream.
The human peptidetransporter is a low affinity, high capacity oligopeptide
transporter system that transports a different range of substrate involving
beta- lactam antibiotics and angiotensin converting enzyme ACE inhibitors.
hPept1 Transporter
Localization
Human peptide transporter 1 (PEPT1) is an uptake transporter with a major
role in the absorption of dietary di- and tripeptides from the small intestinal
lumen.
PEPT1 is mainly expressed in the apical plasma membrane of enterocytes in
the small intestine, with increasing expression from duodenum to ileum; in
renal proximal tubular cells of the S1 segment, and in bile duct epithelial cells
[1].
27.
FUNCTIONS:
1. Nutrient Absorption:
• Transports dipeptides and tripeptides from the intestinal lumen into
enterocytes (intestinal cells).
• Works via proton-gradient dependent mechanism :
• Couples H⁺ ions (protons) with peptide uptake (symport).
2. Drug Transport (Pharmacological Role):
• Recognizes and transports peptide-mimicking drugs, improving their oral
bioavailability .
28.
3. Renal Reabsorption:
• In the kidney (proximal tubule), HPEPT1 reabsorbs peptides from
the glomerular filtrate, helping to conserve nitrogen.
Examples of drugs absorbed via HPEPT1:
• β-lactam antibiotics (e.g., cefadroxil, amoxicillin)
• ACE inhibitors (e.g., enalapril)
• Antiviral prodrugs (e.g., valacyclovir)
• Enables absorption of these drugs across the intestinal barrier.
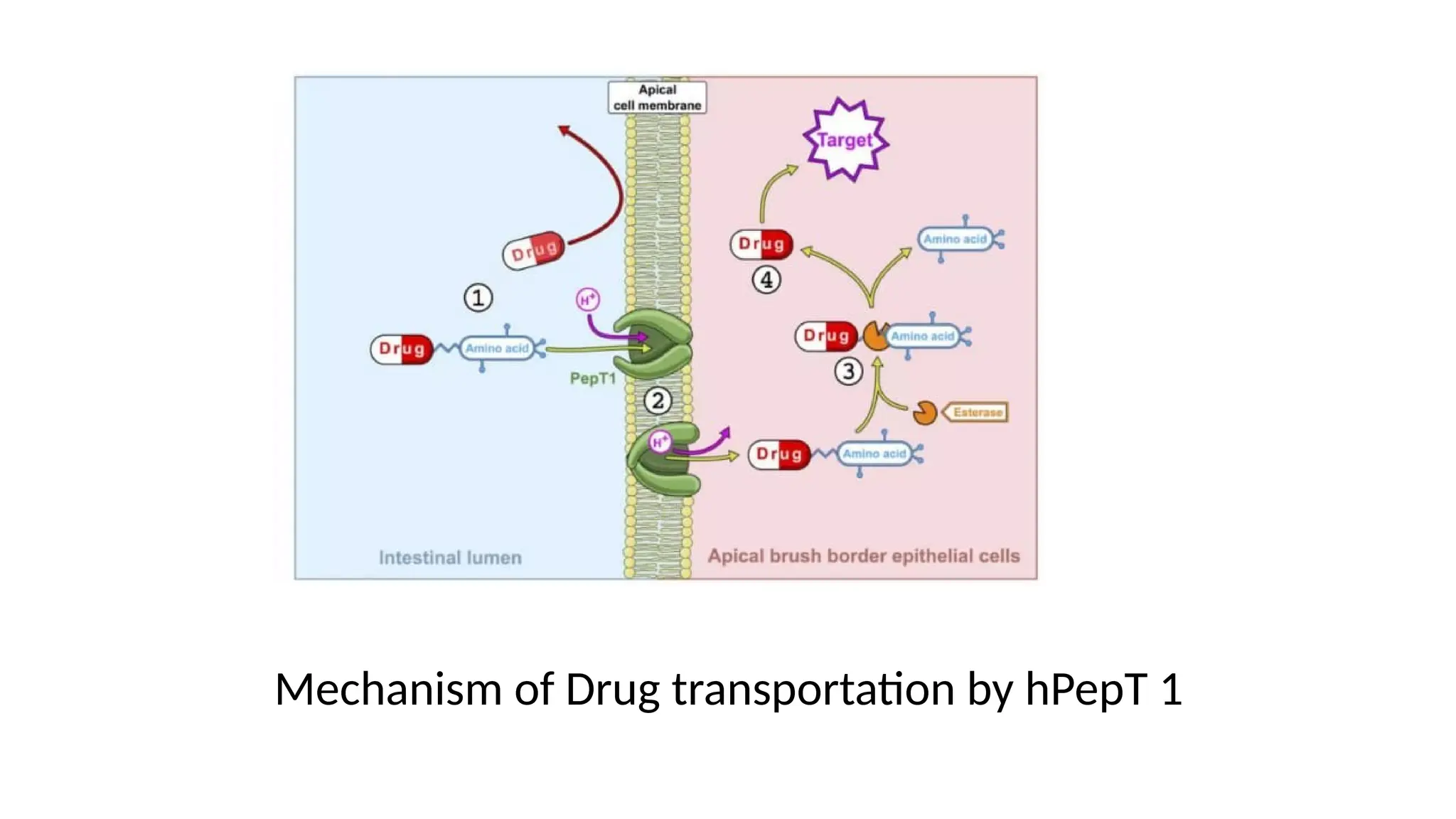
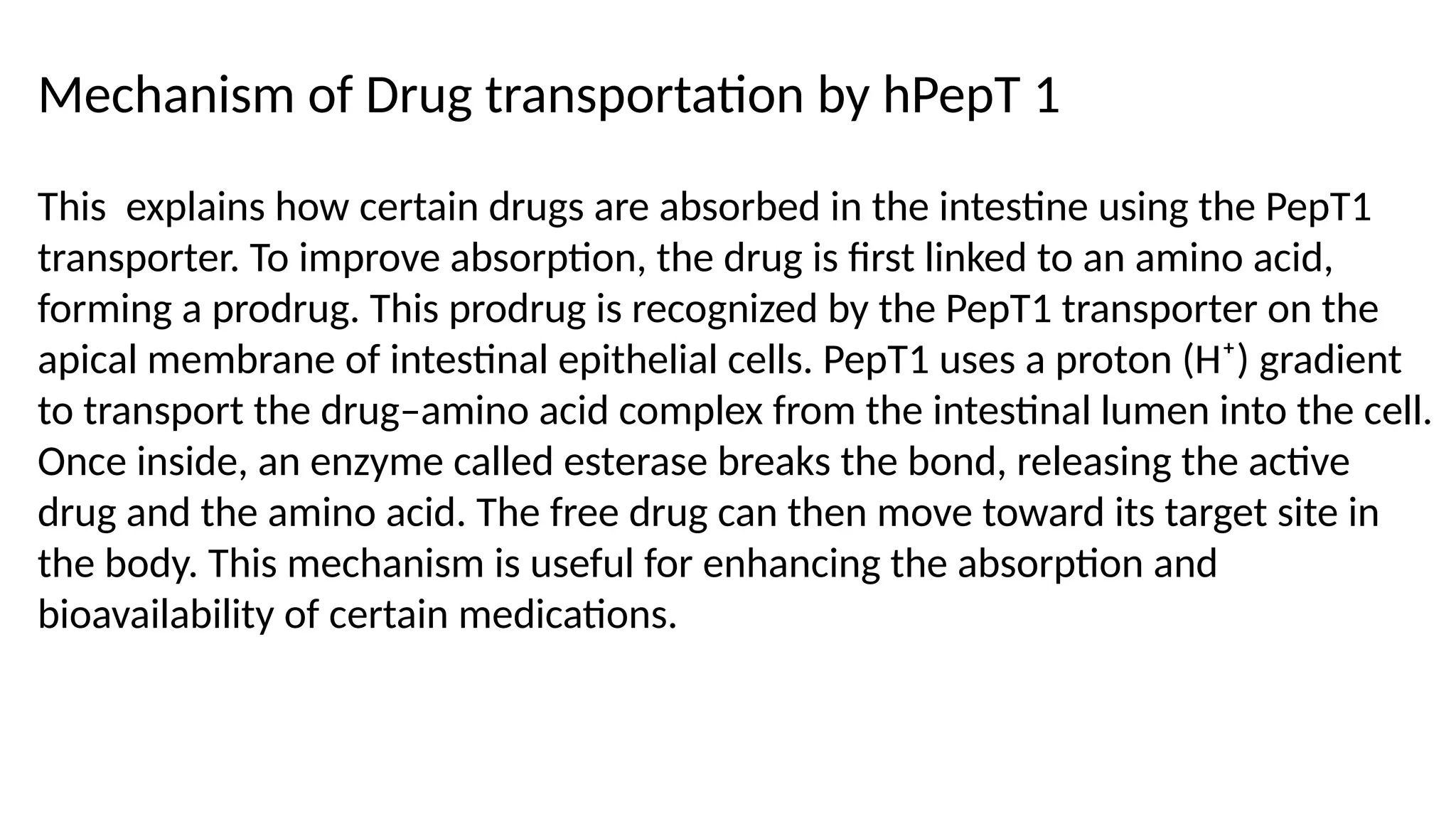
This explains howcertain drugs are absorbed in the intestine using the PepT1
transporter. To improve absorption, the drug is first linked to an amino acid,
forming a prodrug. This prodrug is recognized by the PepT1 transporter on the
apical membrane of intestinal epithelial cells. PepT1 uses a proton (H⁺) gradient
to transport the drug–amino acid complex from the intestinal lumen into the cell.
Once inside, an enzyme called esterase breaks the bond, releasing the active
drug and the amino acid. The free drug can then move toward its target site in
the body. This mechanism is useful for enhancing the absorption and
bioavailability of certain medications.
Mechanism of Drug transportation by hPepT 1
NUCLEOSIDE TRANSPORTERS [NT]
•Nucleoside transporters are specialized proteins found in the cell
membrane that facilitate the movement of nucleosides like adenosine,
cytidine, uridine into and out of the cell . This transporters are essential
for maintain cellular nucleotide pools and enabling the uptake of
nucleoside based drugs.
• Nucleoside transporters transport both naturally occurring nucleosides
and synthetic nucleoside analogs that are used as anticancer drugs and
antiviral drugs.
33.
• There aredifferent types of nucleoside transporters,
• including concentrative nucleoside transporters (CNT1, CNT2, CNT3)
and equilibrative nucleoside transporters (ENT1,ENT2), each having
different substrate specificities.
• concentrative nucleoside transporters having high affinity, where as ENT
having low affinity
34.
• CONCENTRATIVE NUCLEOSIDETRANSPORTERS (CNT)
• CNT consists of three subtypes CNT1, CNT2, CNT3
• These are comprised of 13 Predicted TMD and exhibits several protein
kinase C phosphorylation sites.
• They have wide range of substrate specificities
• e.g. purine adenosine, uridine and purine nucleotides.
• Pharmaceutical compounds include nucleoside analogues
• Ex- zidovudine, lamivudine, cytidine etc.
35.
LOCALIZATION
• CNT expressionhas been shown in small intestine, kidney, liver, heart, brain,
placenta, pancreas, skeletal muscle, colon, rectum, mammary gland, bone
marrow, trachea.
EQUILIBRATIVE NUCLEOSIDE TRANSPORTER (ENT)
• ENT consist of four subtypes ENT1, ENT2, ENT3, ENT4.
• They are characterized by 11 Predicted TMD ENT transport is mediated via a bi-
directional facilitated diffusion mechanism which is dependent upon substrate
concentration gradient.
LOCALIZATION
• ENT is expressed in Liver, Kidney, Lungs, Placenta, CNS Plasma membrane
36.
FUNCTIONS OF NUCLEOSIDETRANSPORTERS
• Transport of Nucleosides and Nucleobases
• Drug Transport and Pharmacokinetics
• Transport of Nucleoside Analogs
BREAST CANCER RESISTANCEPROTEIN [BCRP]
• Breast cancer resistance protein (BCRP)is another ATP-dependent efflux
transporter that confers resistance to a variety of anticancer agents,
including anthracyclines and mitoxantrone, in addition to a high level of
expression in hematological malignancies and solid tumors.
• BCRP is also expressed in intestine, liver and brain , thus implicating its
intricate role in drug disposition behavior.
39.
BCRP
• Recently, Zhangand colleagues generated a BCRP 3D-QSAR model by
analyzing structure and activity of 25 flavonoid analogs. The model
emphasizes very specific structural feature requirements for BCRP such as
the presence of a 2,3-double bond in ring C and hydroxylation at position 5.
• Because the model is only based on a set of closely related structures instead
of a diverse set, it should be applied with caution. Satisfying the transport
model would render a compound susceptible to BCRP, but not fitting into the
model doesn't necessarily exclude the candidate from BCRP transport.
40.
BCRP
• In fact,this caveat should be considered for all predictive in-silico models,
because no model can cover all possible chemical space.
• BCRP is a membrane of the ABC transpoter family has only ATP-binding
cassette and six trans membrane domins, suggesting that BCRP is a half
transporters, which may function as a homo or hetero dimer.
• It plays a role in the secretion of Topotecan.
41.
Absorption :
• IntestinalAbsorption : BCRP is highly expressed in the epithelial cells
lining the small intestine. It acts as an efflux transporter, actively pumping
drugs and other substances back into the intestinal lumen, thus limiting their
absorption into the bloodstream. This reduces the oral bioavailability of
BCRP substrates, affecting how much of the drug reaches systemic
circulation.
• First-pass effect : Similar to P-glycoprotein (P-gp), BCRP contributes to
the first-pass effect by transporting drugs back into the intestinal lumen
before they can be absorbed. 25
PHARMACOKINETIC IMPORTANCE
42.
Distribution :
• Blood-BrainBarrier (BBB): BCRP is present at the blood-brain barrier,
where it limits the entry of drugs into the central nervous system (CNS).
• Placental barrier : BCRP is expressed in the placenta, where it limits
the transfer of drugs and xenobiotics from the maternal circulation to the
fetus
43.
Metabolism :
• Intractionwith drug metabolizing enzymes : BCRP itself is not directly
involved in drug metabolism, it can influence the process by altering the
intracellular concentrations of drugs. By effluxing drugs out of cells.
44.
Excretion :
• RenalExcretion : BCRP is expressed in the renal proximal tubules, where
it facilitates the active secretion of drugs and their metabolites into the urine.
This process is crucial for the elimination of BCRP substrates.
• Biliary Excretion : In the liver, BCRP is involved in the transport of drugs
and metabolites into the bile for excretion. BCRP-mediated biliary excretion
is an important pathway for eliminating certain drugs, particularly those that
are not readily filtered by the kidneys or are too large for passive diffusion.
45.
FUNCTIONS OF BCRP
Drugefflux – pumps out various drugs and xenobiotics.
Protection of tissues
Excretion of metabolites and xenobiotics
46.
REFERENCES
• Computer Applicationsin Pharmaceutical Research and Development
Sean Ekins M.Sc. PhD.
• https://www.slideshare.net/lilycirius/active-transporter
• https://en.wikipedia.org/wiki/Peptide_transporter_1
![P-GP [P-glycoprotein]
• P-glycoprotein (P-GP)is an ATP-dependent efflux transporter that transports a broad
range of substrates out of the cell. It affects drug disposition by reducing absorption
and enhancing renal and hepatic excretion.
• For example, P-GP is known to limit the intestinal absorption of the anticancer drug
Paclitaxel and restricts the CNS penetration of human immune deficiency
virus(HIV)protease inhibitors. It is also responsible for multidrug resistance in cancer
chemotherapy.
• Because of its significance in drug disposition and effective cancer treatment, P-GP
attracted numerous efforts and has become the most extensively studied transporter,
with abundant experimental data.](https://image.slidesharecdn.com/activetransporterspgphpept11-250911101524-ac6c7e9a/75/ACTIVE-TRANSPORTERS-pgp-hpept1-1-pptx-19-2048.jpg)
![The human peptide transporter is a low affinity, high capacity oligopeptide
transporter system that transports a different range of substrate involving
beta- lactam antibiotics and angiotensin converting enzyme ACE inhibitors.
hPept1 Transporter
Localization
Human peptide transporter 1 (PEPT1) is an uptake transporter with a major
role in the absorption of dietary di- and tripeptides from the small intestinal
lumen.
PEPT1 is mainly expressed in the apical plasma membrane of enterocytes in
the small intestine, with increasing expression from duodenum to ileum; in
renal proximal tubular cells of the S1 segment, and in bile duct epithelial cells
[1].](https://image.slidesharecdn.com/activetransporterspgphpept11-250911101524-ac6c7e9a/75/ACTIVE-TRANSPORTERS-pgp-hpept1-1-pptx-26-2048.jpg)
![NUCLEOSIDE TRANSPORTERS [NT]
• Nucleoside transporters are specialized proteins found in the cell
membrane that facilitate the movement of nucleosides like adenosine,
cytidine, uridine into and out of the cell . This transporters are essential
for maintain cellular nucleotide pools and enabling the uptake of
nucleoside based drugs.
• Nucleoside transporters transport both naturally occurring nucleosides
and synthetic nucleoside analogs that are used as anticancer drugs and
antiviral drugs.](https://image.slidesharecdn.com/activetransporterspgphpept11-250911101524-ac6c7e9a/75/ACTIVE-TRANSPORTERS-pgp-hpept1-1-pptx-32-2048.jpg)
![BREAST CANCER RESISTANCE PROTEIN [BCRP]
• Breast cancer resistance protein (BCRP)is another ATP-dependent efflux
transporter that confers resistance to a variety of anticancer agents,
including anthracyclines and mitoxantrone, in addition to a high level of
expression in hematological malignancies and solid tumors.
• BCRP is also expressed in intestine, liver and brain , thus implicating its
intricate role in drug disposition behavior.](https://image.slidesharecdn.com/activetransporterspgphpept11-250911101524-ac6c7e9a/75/ACTIVE-TRANSPORTERS-pgp-hpept1-1-pptx-38-2048.jpg)