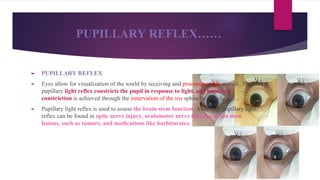
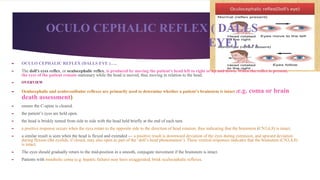
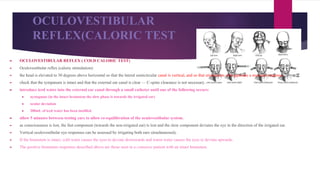
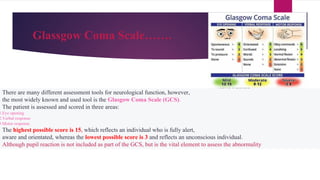
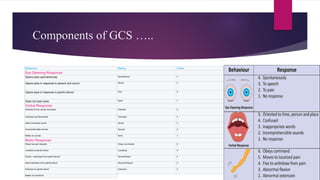
Neurological assessments are important for monitoring patients' neurological status. Key reflexes include pupillary reaction, motor function, and vital signs. The Glasgow Coma Scale assesses eye opening, verbal response, and motor response on a scale of 3 to 15. The AVPU scale rapidly measures consciousness. Pupillary reaction provides information about intracranial pressure and should be round and reactive to light. Motor response examines limb strength. Brainstem reflexes like the pupillary, corneal, gag, cough, doll's eye, and caloric testing help assess brainstem function. The doll's eye reflex checks if eyes remain stationary with head movement while caloric testing assesses eye movement in response to cold water in the ear. Neurological


![INTRA CRANIAL PRESSURE ….
► Elevated intracranial pressure (ICP) is seen in ;
► head trauma, [1]
hydrocephalus, intracranial hemorrhage, sub-arachnoid hemorrhage from ruptured brain
aneurysm, intracranial tumors, [3]
hepatic encephalopathy, [4]
and cerebral edema. Intractable elevated ICP can
lead to death or devastating neurological damage
► either by reducing cerebral perfusion pressure (CPP) [6]
and causing cerebral ischemia or by compressing and causing
herniation of the brainstem or other vital structures. Prompt recognition is crucial in order to intervene appropriately
► CUSHINGS TRIAD…
► refers to a set of signs that are indicative of increased
► intracranial pressure (ICP), or increased pressure in the brain.
► Cushing's triad consists of
► bradycardia (also known as a low heart rate), HR < 50B/MIN
► irregular respirations, some times TACHYPNOEA OR BRADYPNOEA
a widened pulse pressure BP > 150/80MMHG](https://image.slidesharecdn.com/neuroassessmentfornurses-210709034524/85/Neuro-assessment-for-nurses-10-320.jpg)