Downloaded 132 times
![Gas Transport in the Blood
Oxygen transport in the blood
Inside red blood cells attached to
hemoglobin (oxyhemoglobin [HbO2])
A small amount is carried dissolved in the
plasma
Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings](https://image.slidesharecdn.com/mariebch13b-140911080852-phpapp01/85/Marieb-ch13b-5-320.jpg)
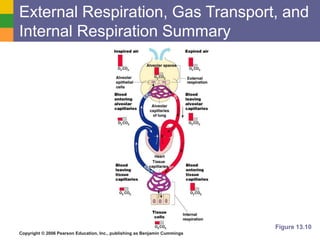
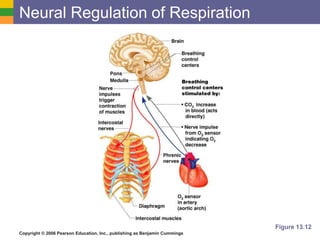

The document discusses several key aspects of respiration, including: 1) External respiration involves the diffusion of oxygen into the blood and carbon dioxide out of the blood in the lungs. Oxygen is transported in red blood cells attached to hemoglobin, while carbon dioxide is transported primarily as bicarbonate ions in the plasma. 2) Internal respiration is the exchange of gases between the blood and tissues, with oxygen diffusing into tissues and carbon dioxide diffusing out. 3) Respiratory rate and depth are regulated by the medulla oblongata and influenced by physical, emotional, and chemical factors like carbon dioxide and oxygen levels in the blood.