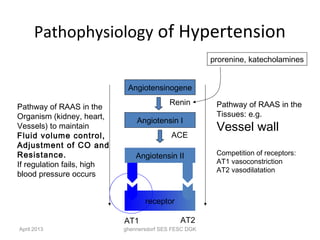
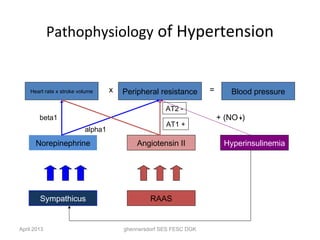
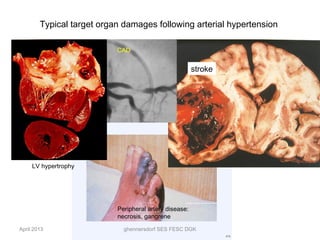
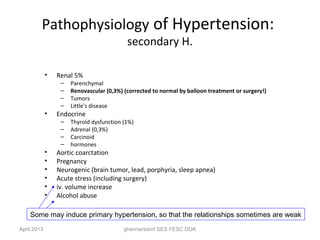
Primary hypertension accounts for 90% of hypertension cases. It is defined as high blood pressure without an identifiable secondary cause. The main pathophysiological drivers of primary hypertension are an overactive renin-angiotensin-aldosterone system and endothelial dysfunction. This leads to increased peripheral resistance and higher blood pressure. Over time, uncontrolled high blood pressure can damage target organs like the heart, brain, kidneys, and blood vessels, potentially causing complications like heart failure, stroke, and kidney disease. Managing risk factors and treating hypertension can help prevent its progression and reduce complications.