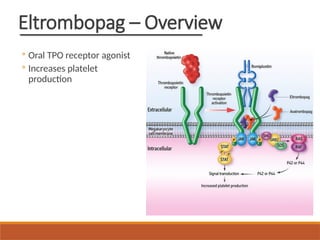
Ianalumab plus
Eltrombopag inImmune
Thrombocytopenia
MODERATOR : DR DEEPJYOTI SAIKIA SIR
ASSISTANT PROFESSOR
DEPT OF GENERAL MEDICINE
PRESENTED BY : DR BIKARNA CHOWDHURY
(PGT 1ST YEAR)
2.
Background – Immune
Thrombocytopenia
Immunethrombocytopenic purpura (ITP) is an acquired
autoimmune disorder characterized by:
• Isolated thrombocytopenia (platelet count <100,000/µL)
• Normal bone marrow (or increased megakaryocytes)
• Absence of other causes of thrombocytopenia
It results from immune-mediated platelet destruction and
impaired platelet production.
3.
Epidemiology and Burden
oRare but chronic disease
o Incidence: 2–5 per 100,000/year
o Children: Often acute, post-viral, self-limiting
o Adults: Chronic, relapsing course
o Slight female predominance in adults
o High relapse rates with Long-term treatment
burden
4.
Current Treatment Goals
◦Prevent bleeding
◦ Maintain safe platelet count
◦ Minimize adverse effects
◦ Improve quality of life
5.
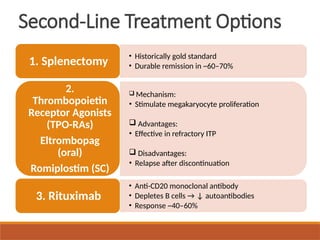
First-Line Therapy
• Prednisone:1 mg/kg/day for 2–4 weeks, then taper
OR
• Dexamethasone: 40 mg/day × 4 days (pulse therapy)
1. Corticosteroids (Mainstay)
• Dose: 1-2 g/kg total given over 1–5 days
• Rapid rise in platelets (24–48 h)
2. Intravenous Immunoglobulin (IVIG)
Unmet Needs inITP
◦ Durable remission lacking
◦ Treatment dependency common
◦ Cumulative toxicity
◦ Need for disease-modifying therapy
8.
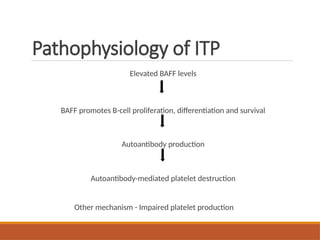
Pathophysiology of ITP
ElevatedBAFF levels
BAFF promotes B-cell proliferation, differentiation and survival
Autoantibody production
Autoantibody-mediated platelet destruction
Other mechanism - Impaired platelet production
9.
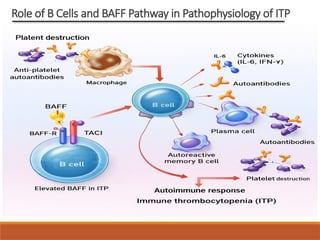
Role of BCells and BAFF Pathway in Pathophysiology of ITP
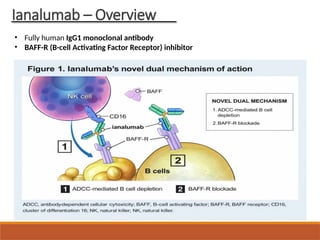
Rationale for Combination
Therapy
◦Suppress autoimmunity with ianalumab
◦ Support platelet production with eltrombopag
◦ Aim for sustained remission
◦ Short-course therapy
13.
Study Objectives
◦ Evaluateefficacy of ianalumab
◦ Assess safety profile
◦ Compare two doses
◦ Measure sustained response
14.
Study Design &Mode of
conduction of Study
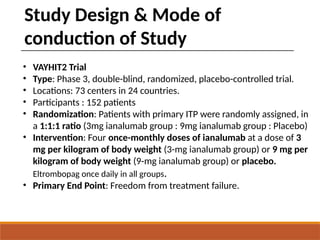
• VAYHIT2 Trial
• Type: Phase 3, double-blind, randomized, placebo-controlled trial.
• Locations: 73 centers in 24 countries.
• Participants : 152 patients
• Randomization: Patients with primary ITP were randomly assigned, in
a 1:1:1 ratio (3mg ianalumab group : 9mg ianalumab group : Placebo)
• Intervention: Four once-monthly doses of ianalumab at a dose of 3
mg per kilogram of body weight (3-mg ianalumab group) or 9 mg per
kilogram of body weight (9-mg ianalumab group) or placebo.
Eltrombopag once daily in all groups.
• Primary End Point: Freedom from treatment failure.
16.
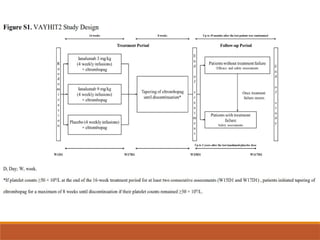
Inclusion criteria
Patients wereeligible if they met all of the following:
1. Age ≥18 years
2. Diagnosis of primary immune thrombocytopenia (ITP)
3. Insufficient response or relapse after first-line glucocorticoid therapy,
defined as:
◦ Insufficient response:
◦ Platelet count <30 × 10⁹/L, OR
◦ Need for glucocorticoids for >8 weeks
◦ Relapse:
◦ Platelet count <30 × 10⁹/L after an initial response to steroids
4. Eligible for treatment with eltrombopag
5. No prior second-line therapy
17.
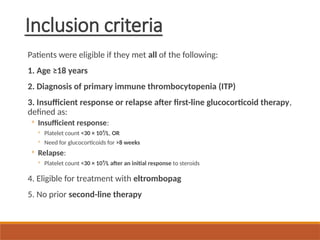
Exclusion criteria
Patients wereexcluded if they had:
1. Received any second-line ITP therapy other than glucocorticoids, including:
◦ Rituximab
◦ Long-term thrombopoietin receptor agonists
◦ Other immunosuppressive or disease-modifying therapies
Exception allowed:
◦ Prior use of a TPO-receptor agonist for ≤7 days before screening was permitted
2. Inadequate dose or duration of first-line glucocorticoid therapy before
randomization
18.
Primary End Point
Freedom from treatment failure determined in a time-to-
event analysis with treatment failure defined by -
◦ Platelet count <30,000/microlitre more than 8 weeks after
randomization
◦ initiation of rescue therapy more than 8 weeks after
randomization
◦ inititiation of new ITP therapy
◦ inability to taper or discontinue Eltrombopag because of
inadequate platelet count
◦ death from any cause
Follow-up up to 12 months
19.
Key Secondary EndPoint
Stable response at 6 months defined by Platelets count
≥50,000/µL at ≥75% measurements from the weeks 19
through 25 without the use of rescue therapy.
Other Secondary End Points
A response (platelet count of ≥50,000/microliter without
use of rescue treatment or new ITP therapy).
A complete response (platelet count of
≥1,00,000/microliter without use of rescue treatment or
new ITP therapy).
Successful tapering or discontinuation of Eltrombopag.
Bleeding events as assessed by WHO bleeding .
The degree and duration of B cell depletion.
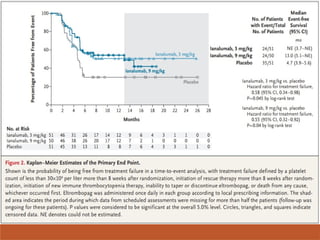
Primary Outcome –Results
Both Ianalumab doses led to a significantly longer
time to treatment failure than placebo
◦ HR for treatment failure (Ianalumab vs placebo) -
0.55 (9 mg/kg group)
◦ HR for treatment failure (Ianalumab vs placebo) -
0.58 (3 mg/kg group)
◦ P < 0.05
22.
Kaplan–Meier Analysis
◦ Higherevent-free survival
◦ Sustained benefit at 12 months
◦ Both doses superior to placebo
◦ Clinically meaningful effect
24.
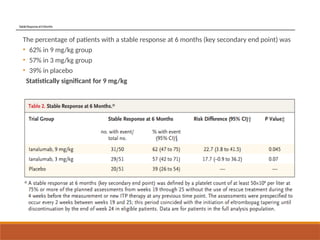
StableResponseat6Months
The percentage ofpatients with a stable response at 6 months (key secondary end point) was
• 62% in 9 mg/kg group
• 57% in 3 mg/kg group
• 39% in placebo
Statistically significant for 9 mg/kg
25.
Eltrombopag Tapering
At 6months after randomization, the Kaplan– Meier estimate of the
probability of having a successful taper and then discontinuing
eltrombopag while maintaining a platelet count of at least 30×109
per liter was
◦ 59% (95% CI, 44 to 71) in the 9-mg ianalumab group,
◦ 60% (95% CI, 45 to 72) in the 3-mg ianalumab group, and
◦ 38% (95% CI, 25 to 52) in the placebo group
Higher discontinuation success
Lower cumulative dose
Shorter duration of therapy
Sustained platelet counts
26.
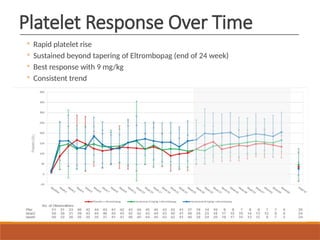
Platelet Response OverTime
◦ Rapid platelet rise
◦ Sustained beyond tapering of Eltrombopag (end of 24 week)
◦ Best response with 9 mg/kg
◦ Consistent trend
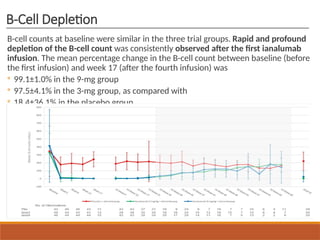
B-Cell Depletion
B-cell countsat baseline were similar in the three trial groups. Rapid and profound
depletion of the B-cell count was consistently observed after the first ianalumab
infusion. The mean percentage change in the B-cell count between baseline (before
the first infusion) and week 17 (after the fourth infusion) was
◦ 99.1±1.0% in the 9-mg group
◦ 97.5±4.1% in the 3-mg group, as compared with
◦ 18.4±36.1% in the placebo group
29.
Quality of Life– Fatigue
◦ PROMIS fatigue improved
◦ ITP-PAQ scores increased
◦ Early and sustained benefit
◦ Patient-centered outcome
30.
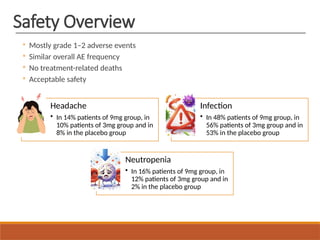
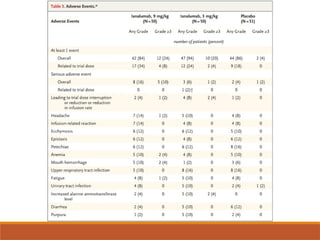
Safety Overview
◦ Mostlygrade 1–2 adverse events
◦ Similar overall AE frequency
◦ No treatment-related deaths
◦ Acceptable safety
Headache
• In 14% patients of 9mg group, in
10% patients of 3mg group and in
8% in the placebo group
Infection
• In 48% patients of 9mg group, in
56% patients of 3mg group and in
53% in the placebo group
Neutropenia
• In 16% patients of 9mg group, in
12% patients of 3mg group and in
2% in the placebo group






















![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)


















