- Family planning, also known as contraception, involves limiting family size and preventing unwanted pregnancy. There are about 1.2 billion women of reproductive age worldwide.
- In Nigeria, the total fertility rate is high at 5.7, leading to high population growth and a doubling of the population every 22 years if trends continue. However, contraceptive use is low, with only 14.6% using any method and 9.7% using modern methods.
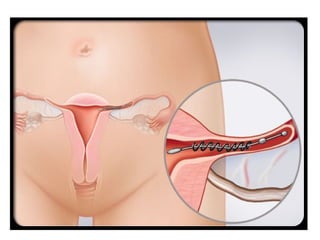
- Family planning methods include natural methods like fertility awareness and lactational amenorrhea, as well as hormonal methods like oral contraceptives, implants, injections, patches, rings, and IUDs. Barrier methods and permanent sterilization procedures










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
