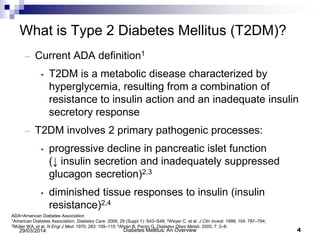
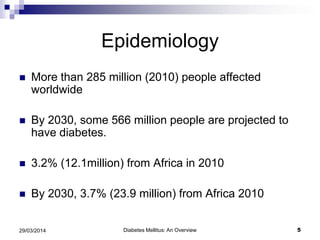
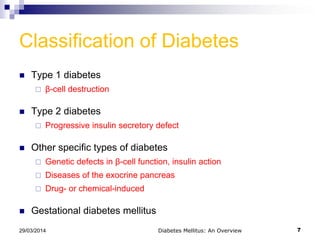
This document provides an overview of diabetes mellitus including its definition, classification, clinical features, investigations, treatment, and complications. It begins with defining the objectives of the lecture which are to define DM, classify its types, list predisposing factors and clinical features, and discuss drugs used in treatment. It then covers epidemiology, the main types of DM including type 1, type 2, and gestational diabetes. Key aspects of diagnosis and management are summarized such as diagnostic criteria, goals of treatment, and approaches including non-pharmacologic, pharmacologic, and surgical options.


![Pharmacology – Amylin Analog
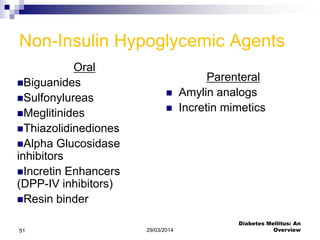
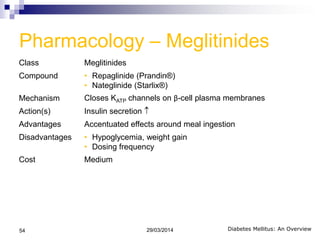
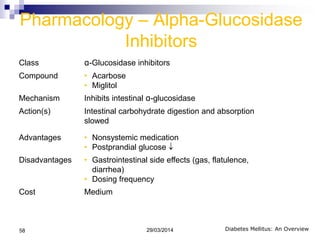
Class Antihyperglycemic Synthetic Analog
Compound • Pramlintide (Symilin®)
Mechanism • Amylinomimetic
Action(s) • Glucagon secretion (glucose-dependent)
• Slows gastric emptying
• Satiety
Advantages • Potential weight loss
Disadvantages • Meal time injections
• Nausea
• Hypoglycemia in combination with insulin
Cost High
Diabetes Mellitus: An Overview
Lexi-Drugs Online [Internet]. Hudson (OH) : Lexi-Comp, Inc. 1978-2012[cited 2012
August 1].
29/03/201463](https://image.slidesharecdn.com/diabetesmellitusanoverview-140329155204-phpapp01/85/Diabetes-mellitus-an-overview-62-320.jpg)







































![D Mmajor[1]](https://cdn.slidesharecdn.com/ss_thumbnails/DMmajor1-123672408595-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













