
More Related Content
What's hot
What's hot (20)
Similar to Management of fistula of ano.
Similar to Management of fistula of ano. (20)
Recently uploaded
Recently uploaded (20)
Management of fistula of ano.
- 1. Dr Paritosh Kumar Singh.
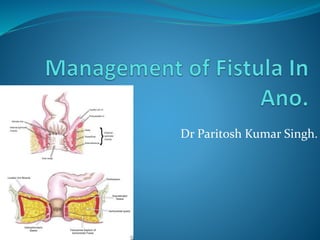
- 2. Introduction: It is a tract lined by granulation tissue which connects perianal skin superficially to anal canal; anorectum or rectum deeply. Etiology: 1. Cryptoglandular(90%) 2. Non cryptoglandular: Tuberculosis, Carcinoma, Crohn’s disease, Ulcerative colitis ,Lymphogranuloma venereum, Hydradenitis suppurativa, Traumatic.
- 3. Classifications: Standard classification: Subcutaneous commonest • Low anal—common • Submucous • High anal • Pelvi-rectal.
- 5. Classifications: It can be. Low level fistulas—these open into the anal canal below the internal ring. High level fistulas—these open into the anal canal at or above the internal ring It can be: Simple fistula without extensions. Complex fistula with extensions. It can be: Single external opening. Multiple external openings which are often seen in tuberculosis,ulcerative colitis, Crohn’s disease, LGV, hidradenitis suppurativa, actinomycosis
- 6. Goodsall’s Rule: Fistulas with an external opening in relation to the anterior half of the anus is of direct type. Fistulas with external openings in relation to posterior half of the anus, has a curved track may be of horse-shoe type, opens in the midline posteriorly and may present with multiple external opening all connected to a single internal opening.
- 7. Investigations: Fistulogram MRI/MRI fistulogram. Endoanal ultrasonography Colonoscopy when IBD is suspected. DRE. EUA. Routine blood investigations.
- 9. Treatment: Goal: Control of sepsis. Eradicate the tract. Minimizing the risk of fecal incontinence, and recurrence
- 10. Fistulectomy: Usually recommended for low anal fistula, as the success rate is high with this procedure, and with minimal incontinence. Success rate 93% to 100%.. Incontinence rate 11.5 to 20%.
- 11. Fistulotomy: After passing the probe through the entire fistulous tract, incision is made over the probe to cut and lay open the fistulous tract. It allows to granulate and heal from the floor/surface. Success rate 93% Risk of incontinence for intersphincteric and trans- sphincteric fistulae is 37% & 54% respectively and higher rate for suprasphincteric and extrasphincteric.
- 13. SETON: Used either for the purpose of cutting sphincter in a phased manner or to mature the tract for another definitive surgery. It is recommended to reduce postoperative fecal incontinence after surgery. Recurrence rate in whom internal sphincter is preserved is 5% and in those sphincter is not preserved is 3%. Overall fecal incontinence rate in internal sphincter preserving is 5.6% and in those of sphincter not preserving is 25.2%.
- 15. Advanced Treatment options for complex fistula Ligation of tract Filling the tract Obliteration of tract. Glue Plug Advancement flap LIFT FiLaC VAAFT
- 16. Anal fistula plug. Made up of synthetic polymer, that provide a scaffold to promote tract healing using sphincter preserving approach. It is positioned from inside the anus with sutures and conforms to the tract. A mucosal flap can be raise and used to cover internal opening. Success rate is 55% for both cryptoglandular and Crohn's fistulae. Complications: Plug dislodgement, infection, or failure with formation of a persistent tract.
- 17. Glue. Made up of fibrinogen, thrombin, and other clotting factors. It is injected into a prepared anal fistula tract to seal it. Healing rate is 50-60%. Results are better in case of simple fistulae. Advantage: simple to use, sphincter sparing, should not effect the later treatment options in the event of its failure. Disadvantage is it high failure rate. Modification: adding stem cells.
- 18. Anorectal advancement flap: • Done for high or complex anal fistulae. • It involves debridement of the fistula tract, utilization of a well-vascularized rectal mucosa or anodermal flap to cover the internal opening of the tract with or without closure of the tract. • The success rate at one year to be 60%. • Repeating the procedure multiple times can further increase the success rate to as much as 90%
- 19. Ligation of Intersphincteric Fistula Tract ( LIFT ). Principle: disconnection of the fistula tract from the anal canal with eradication of the tract in the intersphincteric space. Proc: Involves a radial incision at the intersphincteric groove, with dissection continued cranially in the intersphinteric plane to isolate the fistula tract as it crosses from the internal to the external sphincter. The tract is ligated ( watertight ligation) with absorbable sutures at the lateral border of the internal anal sphincter and the external component is treated by curettage or fistulotomy.
- 20. Drawbacks: This surgery require large tissue dissection so, in case of previous operated patient it will be difficult to identify the tract. This surgery is best suited for patient with simple high trans-sphincteric fistulae of cryptoglandular etiology. Success rate 40 – 95% ( Short term outcomes 71-76%). Modifications: placement of biological graft to reinforce the ligation and closure of the fistula tract( success rate 92%). Use of anal plug to close the external tract in addition to the LIFT procedure. ( success rate 95%, complete healing time 4 weeks). Partial fistulotomy may also be done ( success rate 85%)
- 21. Video assisted anal fistula treatment ( VAAFT). It uses 5mm fistuloscope with 8 degree angled eye piece, Gylycine-mannitol is used to open the fistula tract. Unipolar electrode is used to cauterize the lining of the fistula tract and endobrush is used to extract the necrotic materials. Closure of the internal opening by stapler, suture or advancement flap. Primary healing rate of 74% at 3 months and 87% at the end of 1 year.
- 22. Fistula Laser Closure ( FiLaC ): It uses radial emitting laser probe, drawn through a prepared tract, which destroys the epithelial lining with minimal thermal spread or extra-luminal tissue damage. The internal opening is closed by advancement flap. Data suggest that 71% closure rate at median 20 months follow up with no deterioration in continence.
- 23. Discussion: Fistula plugs and glue have a high failure rate with fistula healing occurring in only ½ of the patients but the risk of sphincter damage is low. The LIFT procedure appears to be a attractive treatment option for cryptoglandular trans-sphincteric fistulae with around 3/4th of patients having successful healing but the results may not be favorable in case of complex or recurrent fistulae. Endoluminal obliteration of the fistula tract using Laser ( FiLaC) or diathermy is a novel approach in the treatment of fistulae with encouraging results in Pilot data, further studies are required before these interventions are adopted into routine clinical practice.
- 24. Thank you..