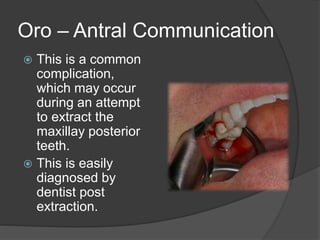
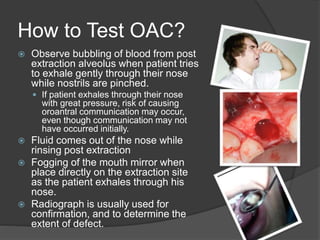
This document discusses the anatomy and pathology of the maxillary sinus and oroantral communications. It describes the location and drainage of the maxillary sinus and causes of sinusitis. Oroantral communications are defined as pathological connections between the oral cavity and maxillary sinus that can form due to dental procedures or trauma. Signs, testing methods, prevention, and management strategies are outlined for both acute communications and oroantral fistulas. Surgical techniques for repair include local soft tissue flaps, grafts, and use of the buccal fat pad flap. Immediate closure of communications less than 3 weeks old has a high success rate, while delayed or recurrent fistulas require surgical intervention.







































![maxillarysinus-170705134531 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinus-170705134531autosaved-240606120847-09cc00a0-thumbnail.jpg?width=640&height=640&fit=bounds)





























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

