Downloaded 119 times


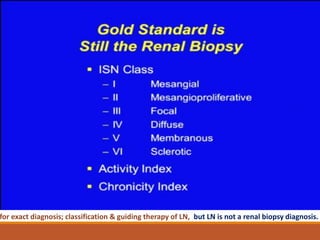
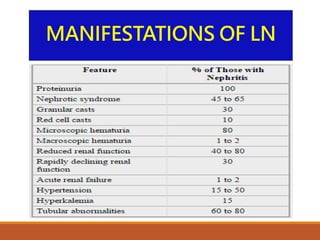
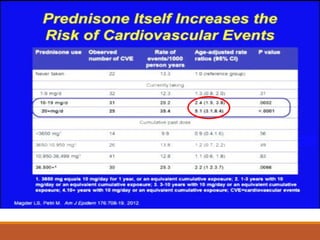
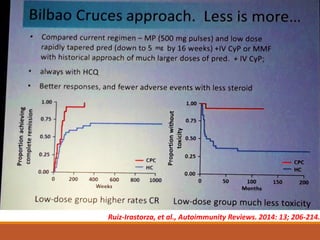

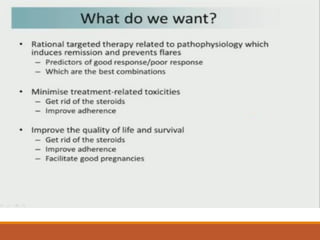



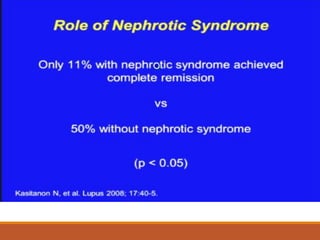
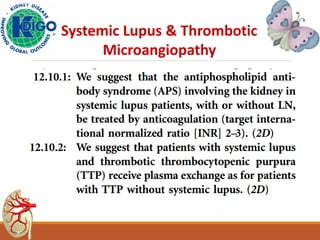




This document discusses lupus nephritis (LN), kidney involvement in systemic lupus erythematosus (SLE). It notes that LN occurs in 50-70% of SLE patients and can range from mild to severe. Despite treatment advances, LN still leads to end-stage renal disease in 17-25% and increased cardiovascular risk. The manifestations and classification of LN are described. Treatment involves immunosuppressants like mycophenolate mofetil and hydroxychloroquine to induce remission while minimizing steroid use. The RITUXILUP protocol at Imperial College London uses rituximab and steroids to achieve remission in LN without long-term oral steroids. Future directions may include










































































































