Download as PDF, PPTX









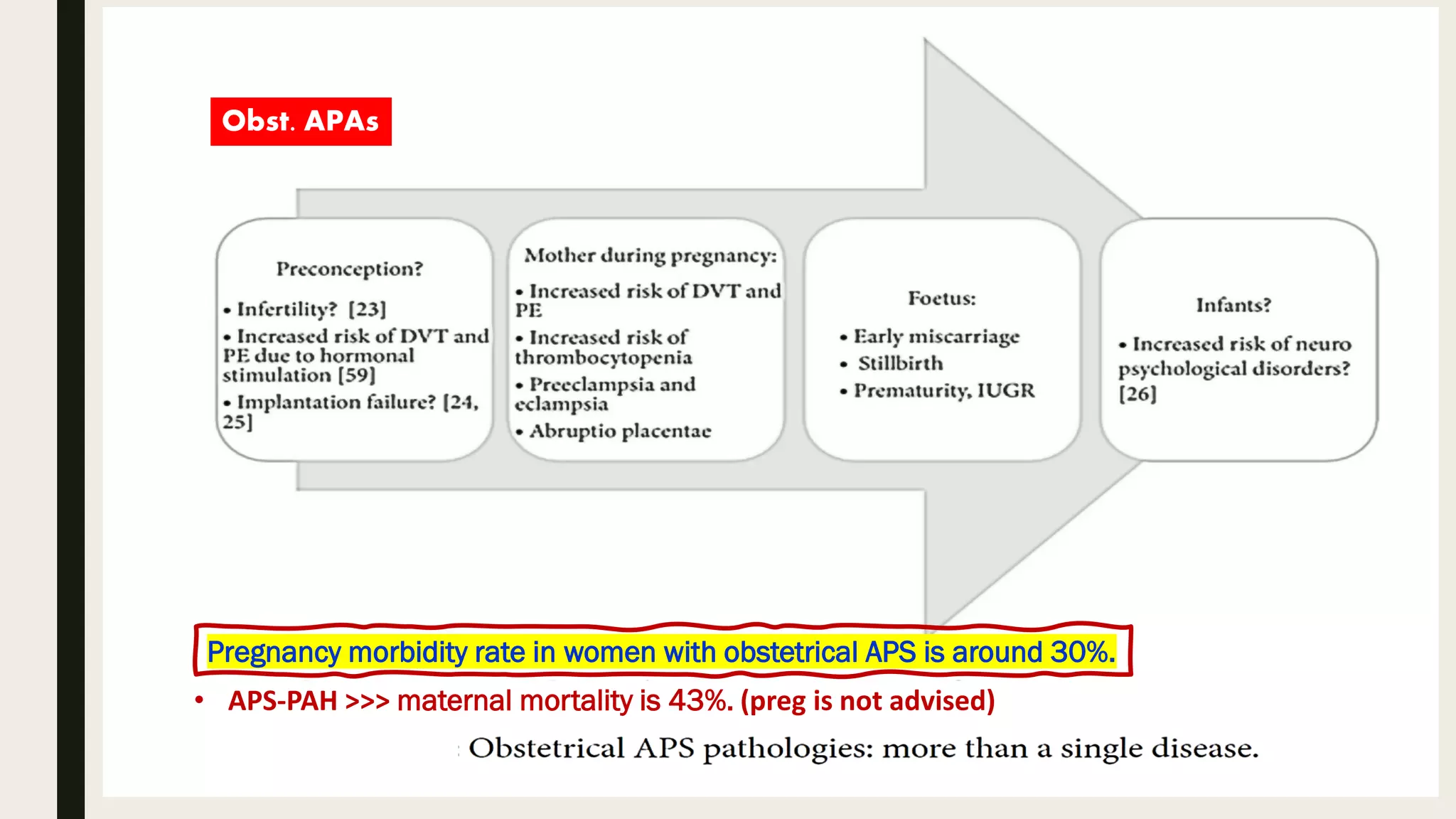













































Antiphospholipid syndrome (APS) is an autoimmune disorder marked by recurrent thrombosis and fetal loss, primarily in females aged 20-40, and can be classified as primary or secondary. The document outlines the pathogenesis, diagnosis, and management strategies for APS, including the role of anticoagulants, risk factors, and specialized treatment for obstetric and catastrophic APS (CAPS). Current guidelines recommend risk stratification and tailored prevention and treatment protocols based on individual patient profiles.