Download as PDF, PPTX
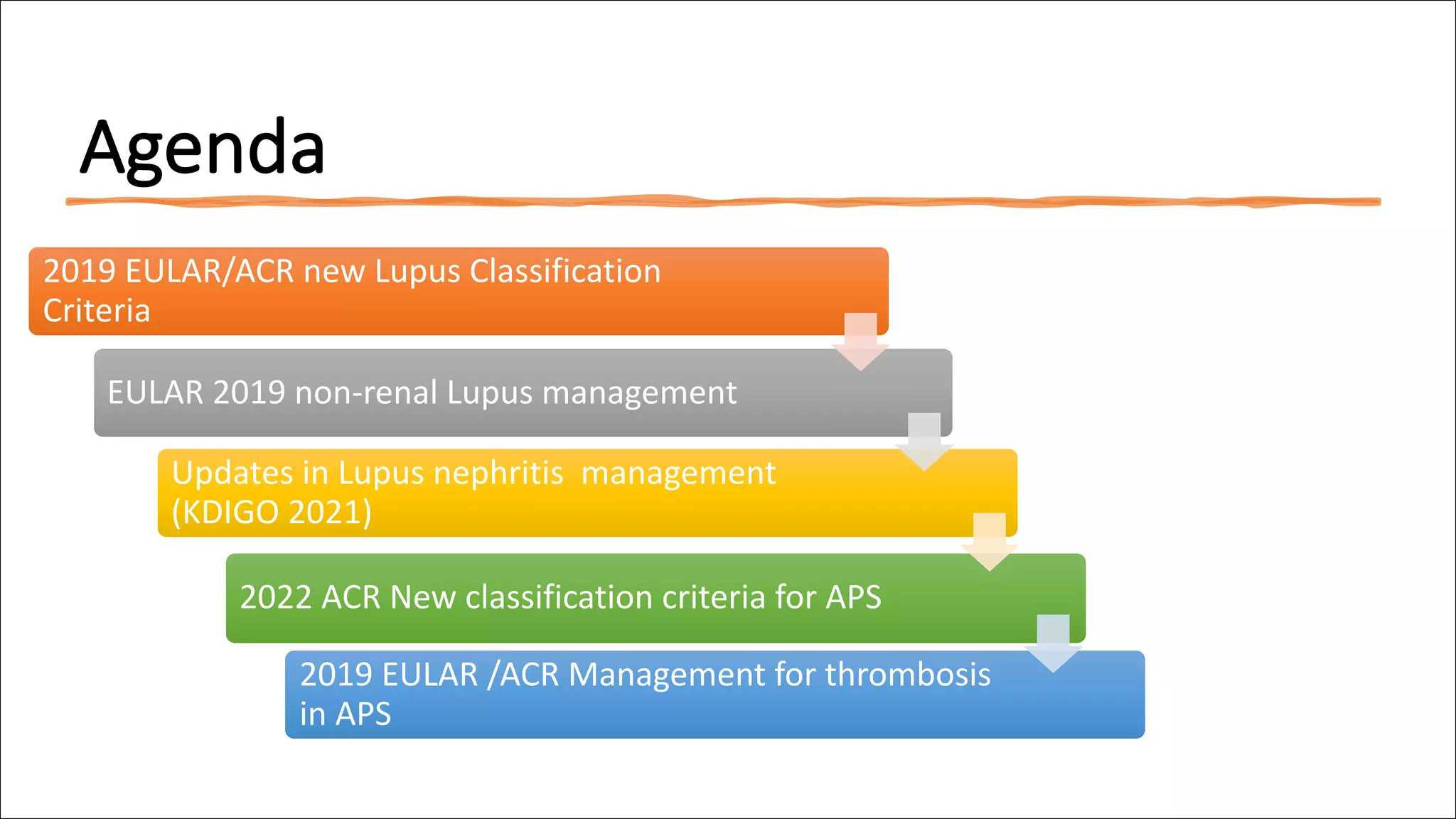





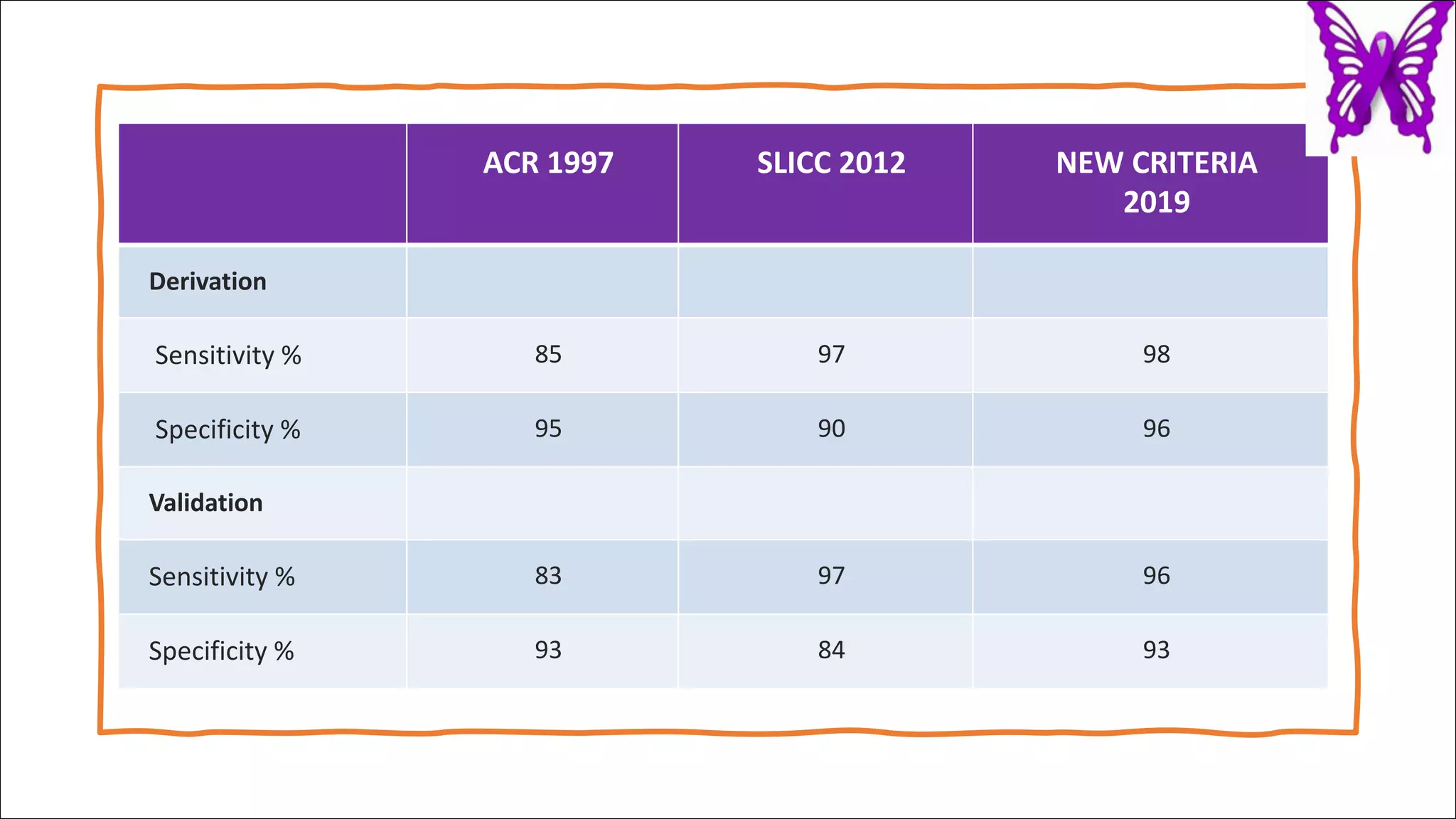


























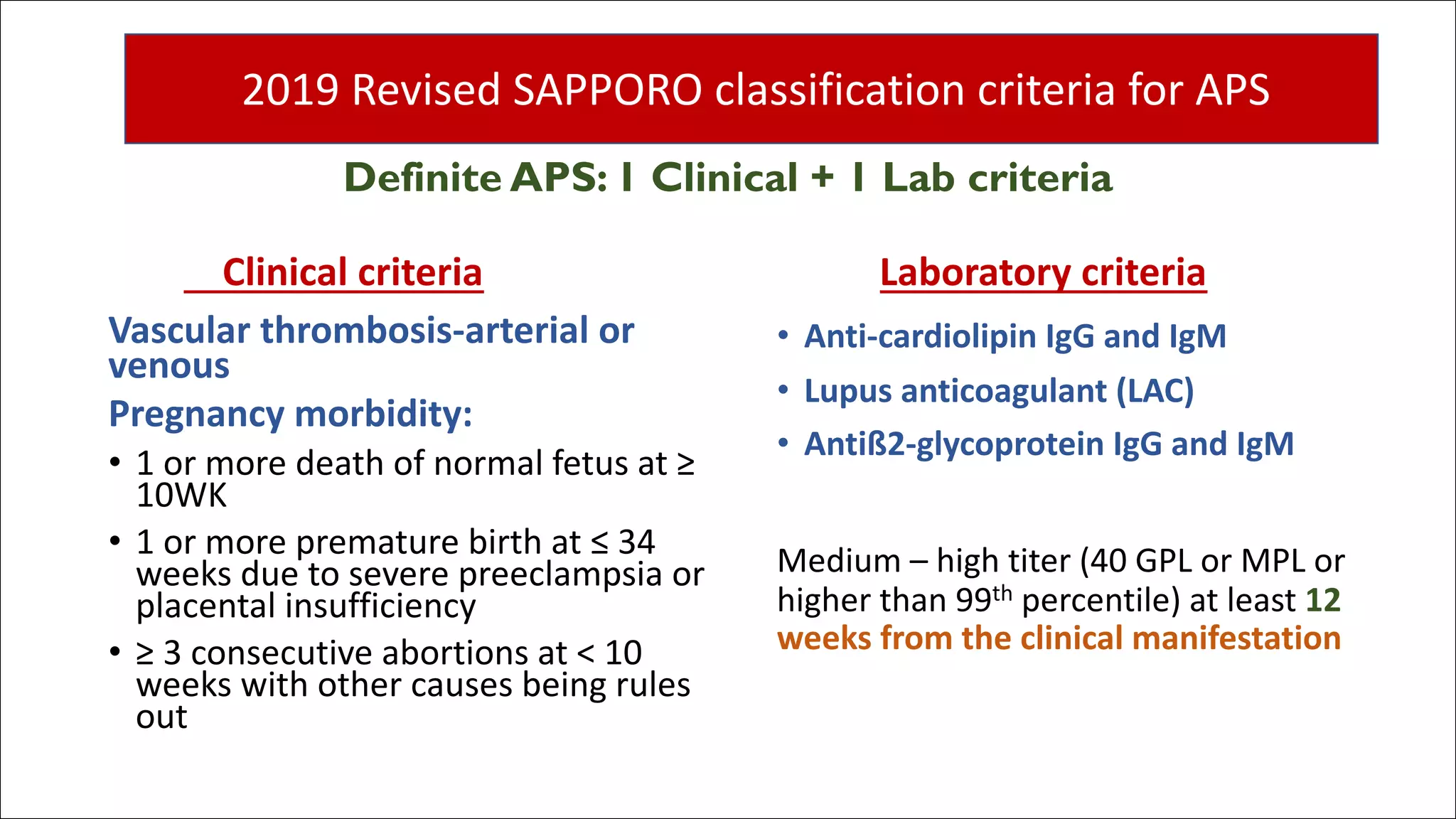


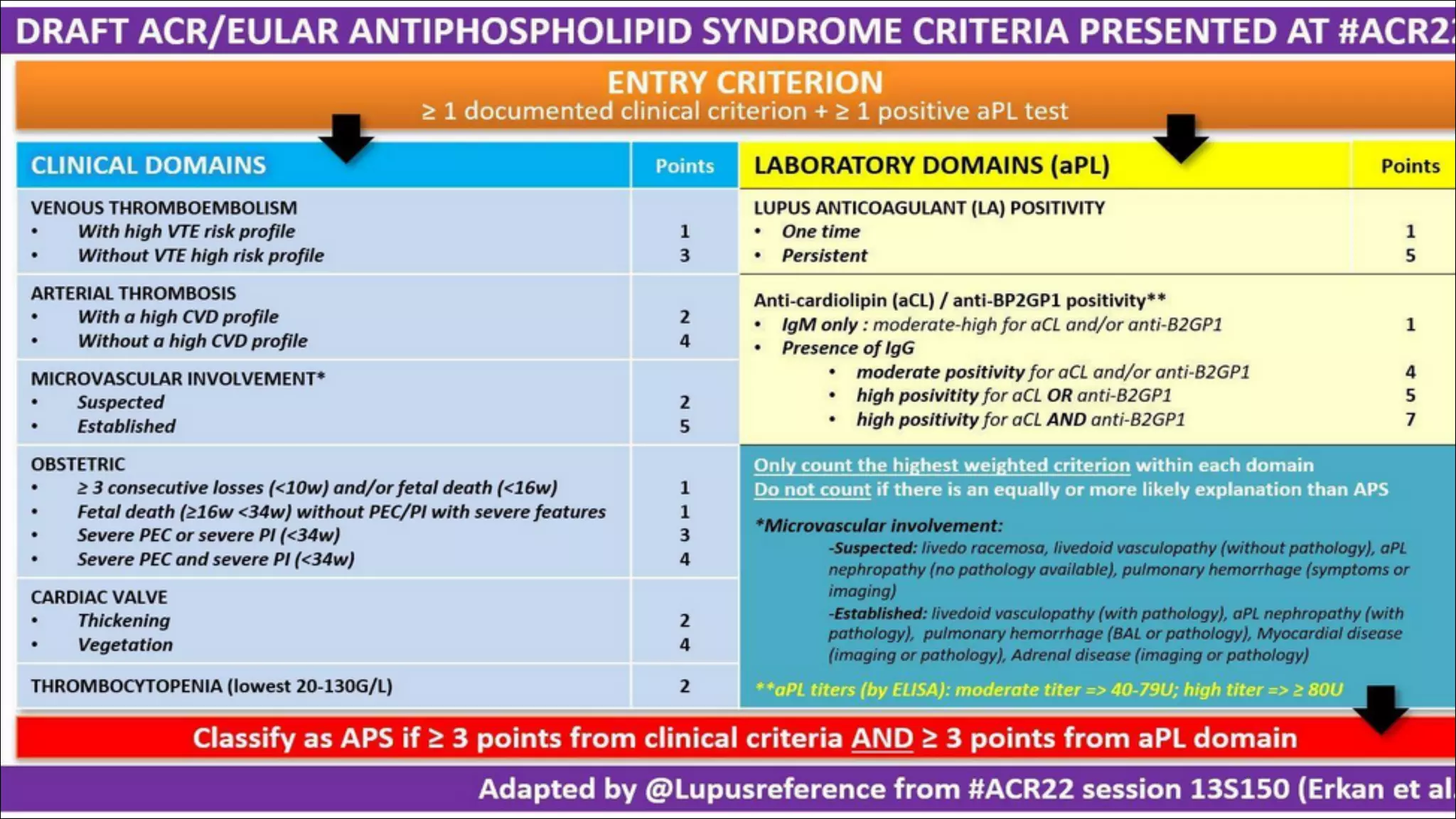


















The document discusses recent advancements in the classification and management of systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS), including updates on the 2019 EULAR/ACR lupus classification criteria and new treatments for lupus nephritis such as belimumab and voclosporin. It elaborates on the implications of various lupus nephritis subtypes and the importance of kidney biopsy for accurate diagnosis, as well as the management recommendations for patients, especially in regard to medications like hydroxychloroquine. Additionally, it highlights the new 2022 APS classification criteria and addresses treatment strategies for both APS and complications during pregnancy.