Downloaded 143 times

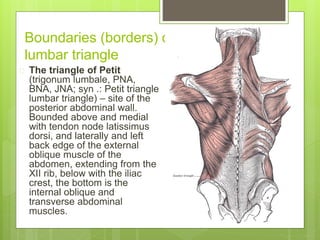



The document discusses the anatomical characteristics of the lumbar triangle, also known as Petit’s triangle, and its relevance in surgery, particularly concerning hernias. Jean-Louis Petit, a French surgeon, is highlighted for his contributions to anatomy and surgical techniques. The document covers the boundaries of the triangle, types of lumbar hernias, treatment methods, and the triangle's surgical significance.















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













