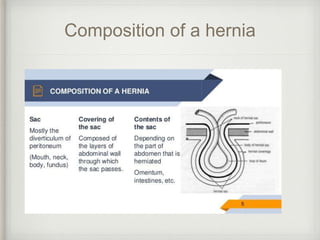
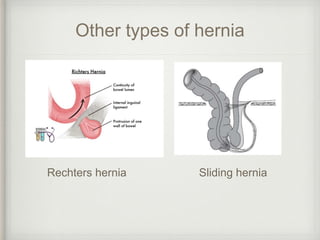
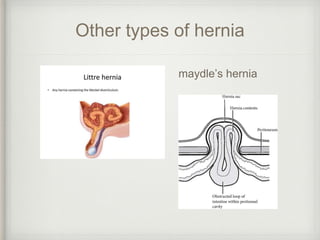
A hernia is a protrusion of an organ or tissue through a weakness in the wall of the cavity it is contained within. Common abdominal hernias include inguinal, umbilical, incisional, femoral, and epigastric hernias. An inguinal hernia, the most common type, can be direct or indirect and occurs when abdominal contents protrude through the inguinal canal. Risk factors for hernias include straining, obesity, pregnancy, coughing, and congenital abnormalities. Hernias can be irreducible, incarcerated, obstructed, or strangulated depending on whether the contents can be reduced and if the blood supply is compromised. Surgical repair options include open tissue or