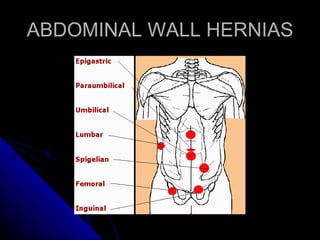
The document discusses various abdominal wall defects including hernias. It describes the anatomy and embryology of the abdominal wall and covers different types of hernias such as umbilical, epigastric, incisional and congenital defects. Diagnosis and repair techniques involving primary closure or mesh are discussed for each type of hernia.