Downloaded 57 times






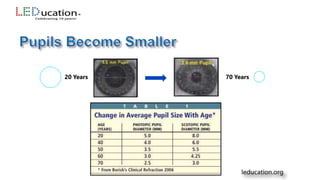

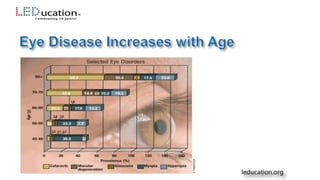
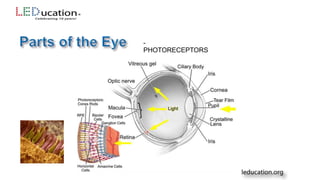
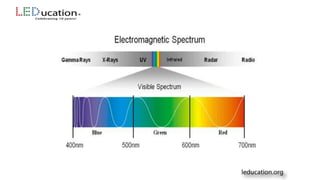




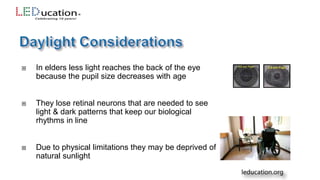
















This presentation discusses the impact of aging on eyesight and how proper lighting can enhance the living conditions of the elderly. It covers the physical changes in the eye with age, common diseases, and evidence-based lighting solutions that improve health and well-being. Participants will learn practical strategies for designing lighting environments that support the visual needs of older adults, including recommendations from the IESNA Lighting Handbook.

























































![Safety for elderly with visual limitations powerpoint video[1]](https://cdn.slidesharecdn.com/ss_thumbnails/safetyforelderlywithvisuallimitationspowerpoint-video1-120310134333-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

































![Getting Started with Apache Spark: Big Data Made Simple [Free Meetup]](https://cdn.slidesharecdn.com/ss_thumbnails/apachesparkgettingstarted-260203175547-8361bcc3-thumbnail.jpg?width=640&height=640&fit=bounds)















