- Airway suction is used to remove secretions from the lungs in intubated patients unable to cough effectively.
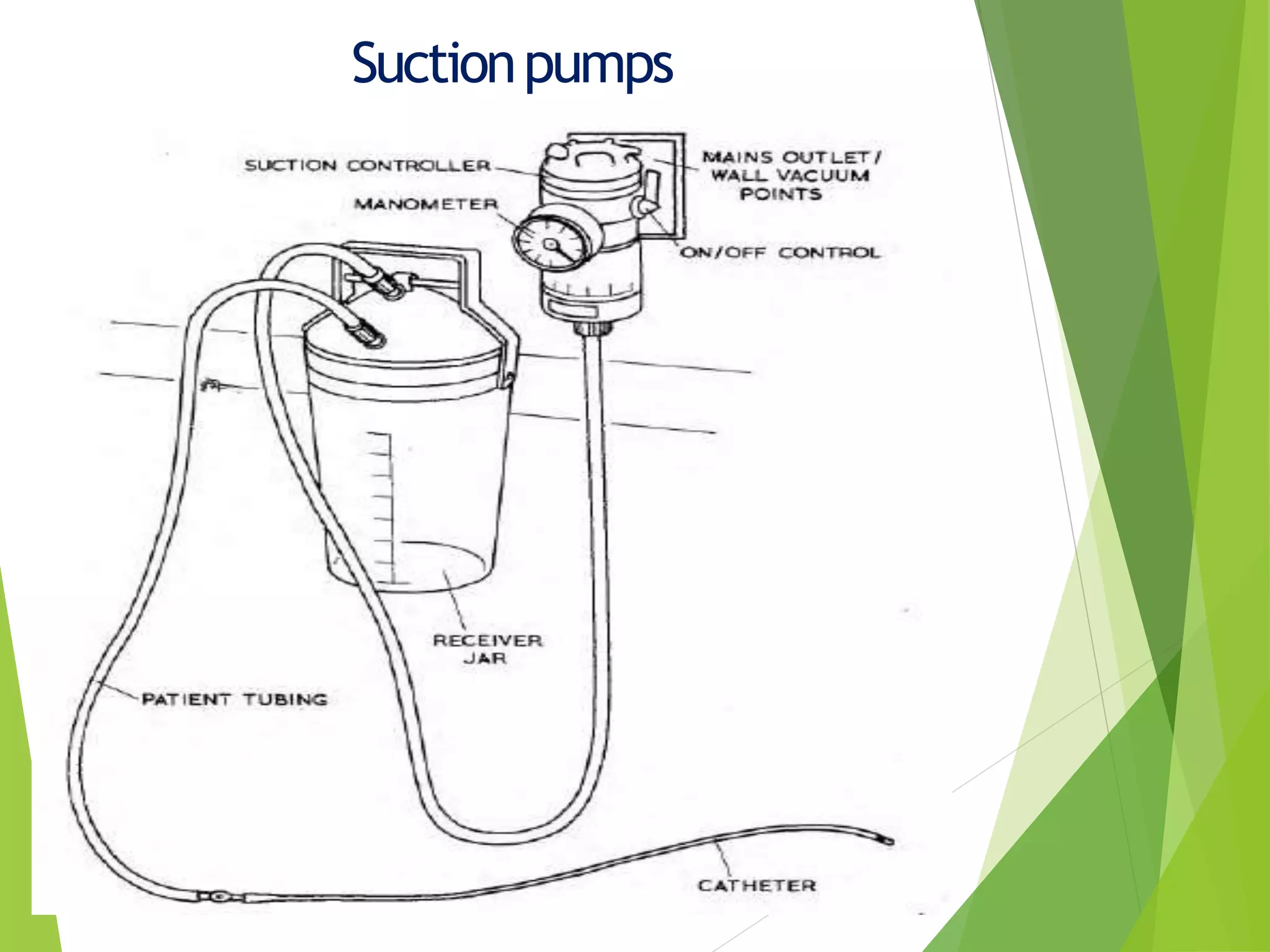
- Proper suction equipment includes pumps, tubing, connections, catheters, and suction trolleys. Pumps can be wall vacuum, electrical, portable, or foot operated.
- Correct suction technique is important to minimize trauma, hypoxia, arrhythmias, atelectasis, and bleeding by using the proper catheter size, intermittent suction, and sterile technique.