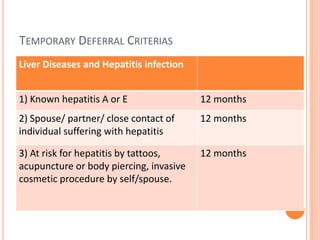
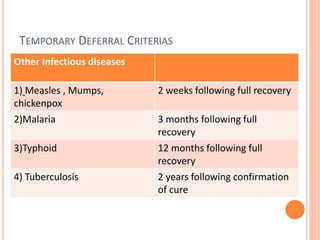
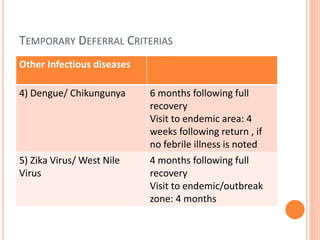
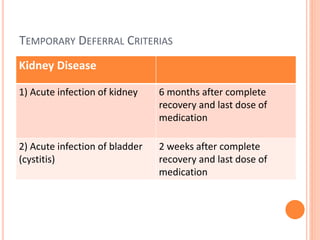
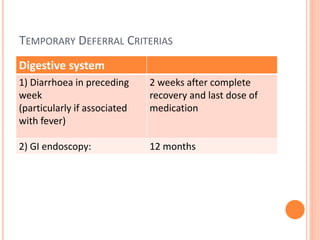
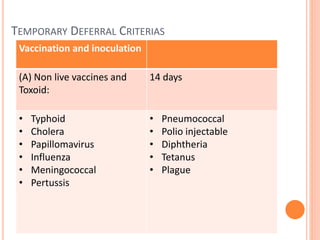
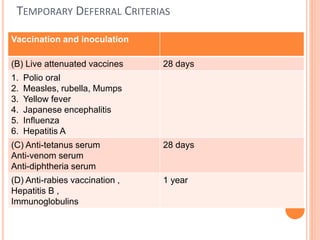
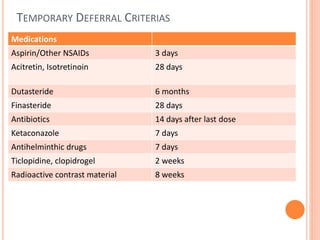
This document discusses donor selection and blood collection procedures. It outlines strategies for donor recruitment including voluntary, social persuasion, and remunerated donations. The donor selection process involves counseling, screening donors using a questionnaire and health check, and determining temporary or permanent deferrals. Blood collection follows standard safety procedures using approved equipment and materials while monitoring the donor's health.