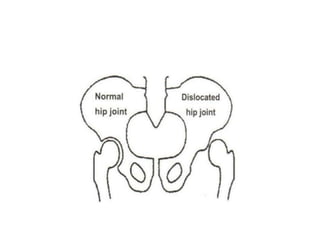
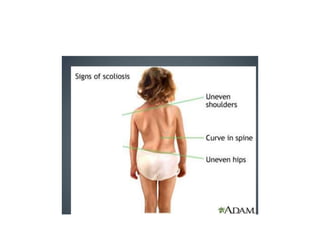
Developmental dysplasia of the hip (DDH) is a condition where the ball and socket joint of the hip do not develop properly. It can affect one or both hips and is more common in females. Treatment depends on the age of the patient, ranging from hip harnesses or splints for young infants to closed or open surgical reduction for older patients. Common spinal deformities discussed include scoliosis, kyphosis, lordosis, torticollis, and flat back. Scoliosis causes an abnormal lateral curvature of the spine. Treatment involves observation, bracing, or surgery depending on the severity of the curvature. Kyphosis and lordosis refer to abnormal curvatures of the thoracic and lumbar