Download as PDF, PPTX
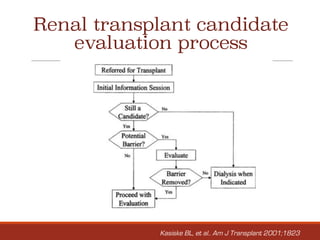
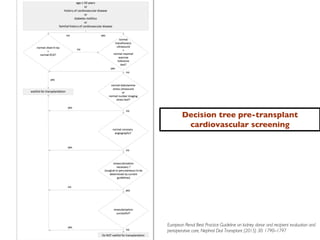



This document provides guidance on evaluating and screening potential renal transplant recipients. It discusses: 1. General concepts to consider include referring all end-stage renal disease patients for transplant evaluation once renal replacement therapy is needed within 12 months, and encouraging preemptive kidney transplantation when feasible. 2. The evaluation process involves assessing medical history and conditions, performing initial screening tests, and evaluating any cardiovascular, infectious, or other systemic diseases to identify any absolute contraindications to transplantation or conditions requiring further treatment and monitoring. 3. Cardiovascular disease is a major cause of death for transplant recipients, so candidates undergo cardiac screening and testing based on risk factors to clear them for surgery or identify any need for pre-operative cardiac










![Human Renal Transplantation [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/humanrenaltransplantationedmond-140716214736-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































































































