Download as PDF, PPTX
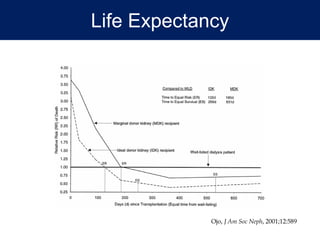
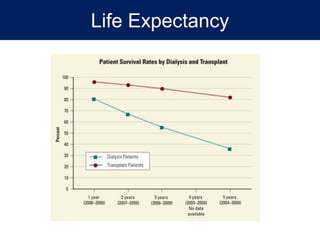
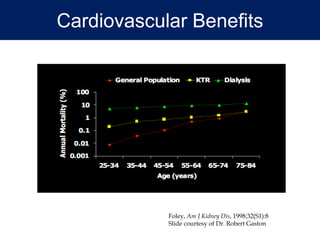




Renal transplantation provides significant benefits over dialysis such as improved life expectancy, cardiovascular health, quality of life, and socioeconomic outcomes. A successful transplant requires careful patient and donor selection as well as lifelong immunosuppression to prevent rejection. Common post-transplant complications include surgical issues, rejection, infection, malignancy, and chronic allograft dysfunction. Close monitoring of recipients and living donors is important to maximize benefits while minimizing risks of this life-saving therapy.
![Human Renal Transplantation [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/humanrenaltransplantationedmond-140716214736-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






















































































