Download as PDF, PPTX
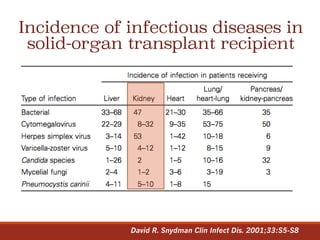
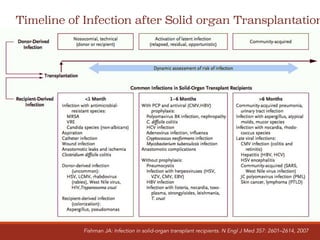
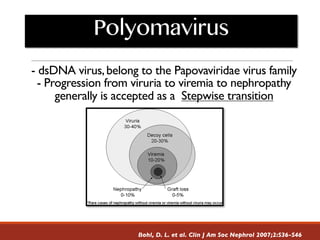
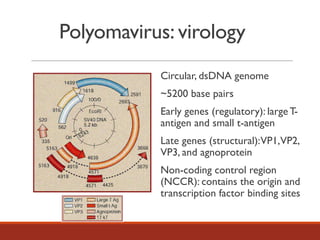
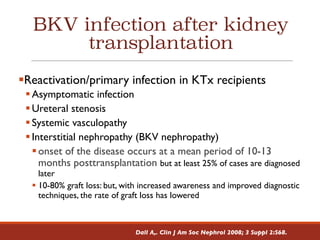
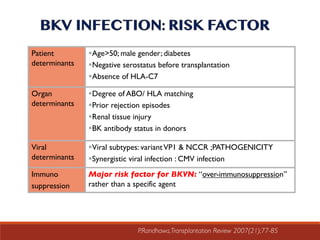
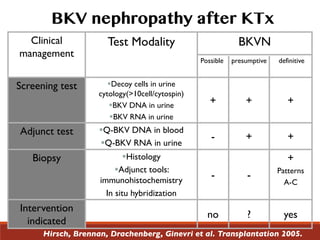
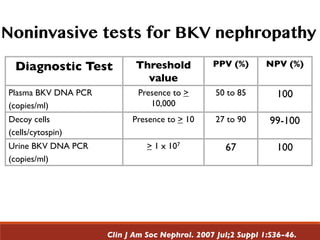
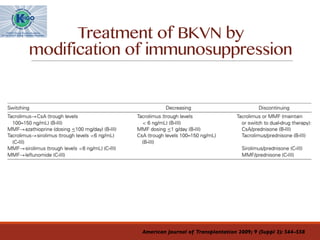
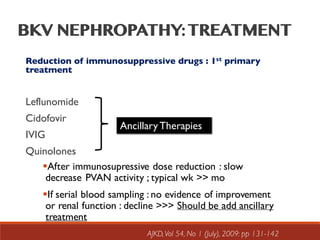
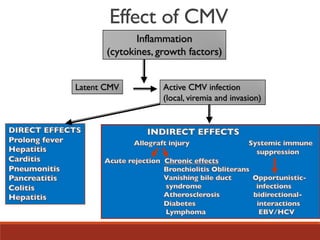
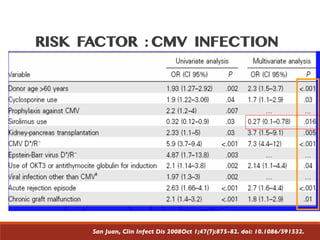
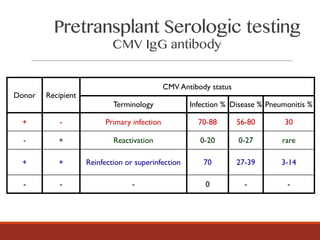
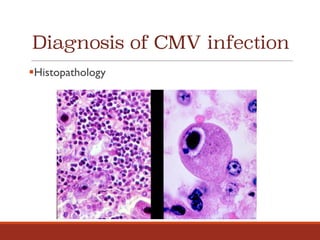


This document discusses infection following renal transplantation. It covers four main categories of exposures that can lead to post-transplant infection: donor-derived, recipient-derived, nosocomial, and community. It then discusses the timeline of various infections, highlighting that CMV and opportunistic infections are most common in the first 6 months. BK virus is also reviewed in depth, including its virology, risk factors for BK virus nephropathy, diagnosis, clinical management and treatment through immunosuppression modification. Cytomegalovirus infection is also summarized, covering terminology, risk factors, diagnostic methods including histopathology, viral culture, serology and molecular assays to detect viral load.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












