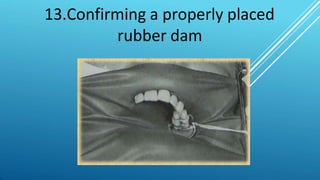
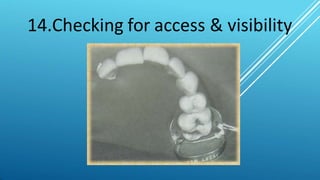
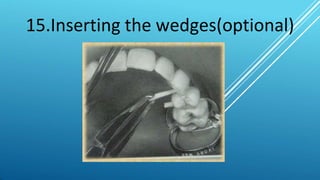
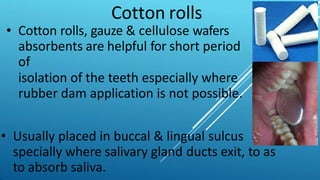
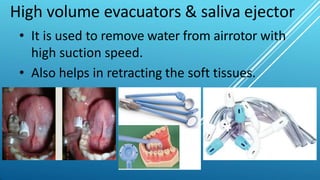
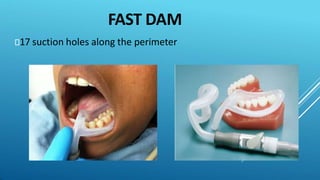
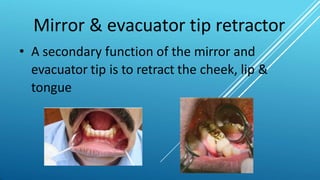
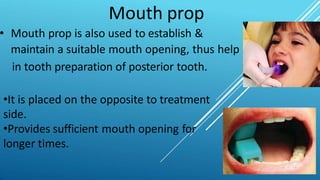
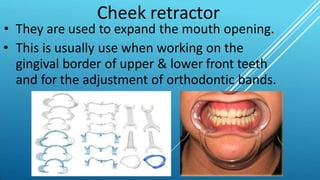
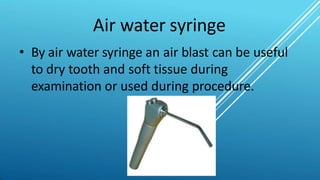
The document discusses isolation of the operative field during dental procedures. Several components must be controlled, including saliva, tongue, and soft tissues. Rubber dam provides the best isolation, allowing a dry, clean field and protecting tissues. Other isolation techniques and materials include cotton rolls, high-volume evacuators, cheek retractors, and air-water syringes. Proper isolation improves visibility, infection control, and material properties during restorative dental work.





















































![Isolation-of-the-operating-field[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/isolation-of-the-operating-field1autosaved-250226051150-dcc1b95b-thumbnail.jpg?width=640&height=640&fit=bounds)











































