Downloaded 2,594 times

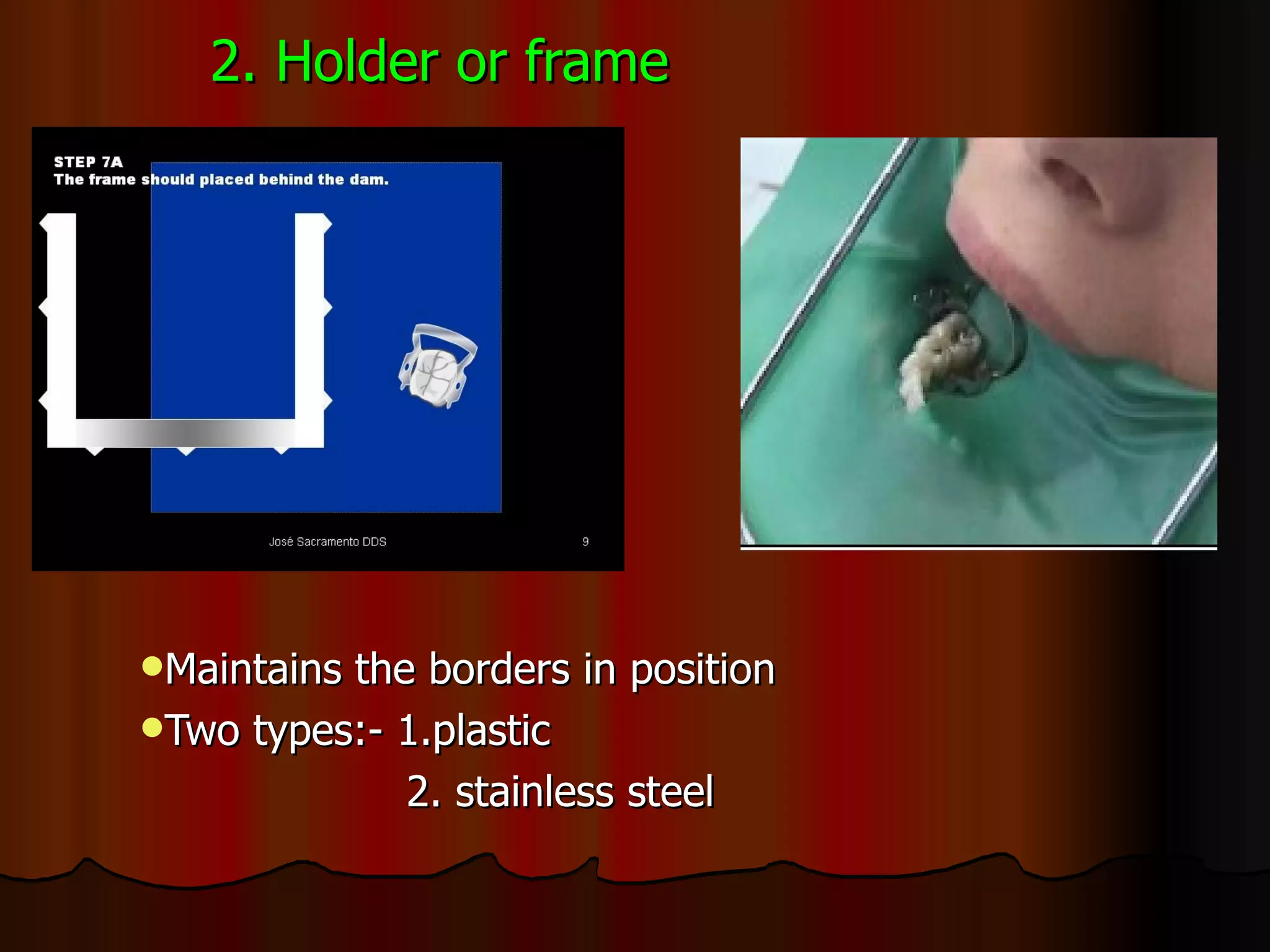


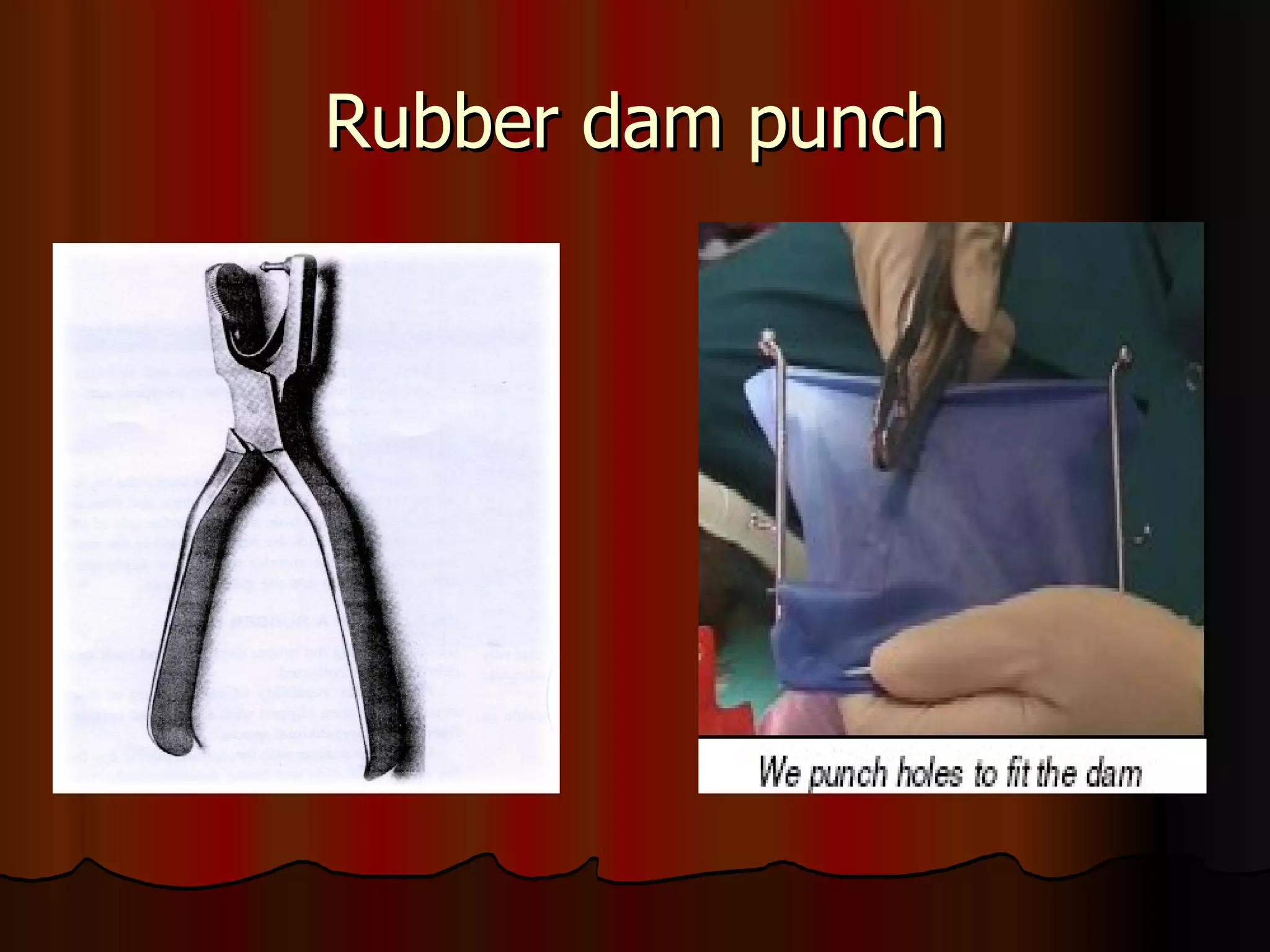
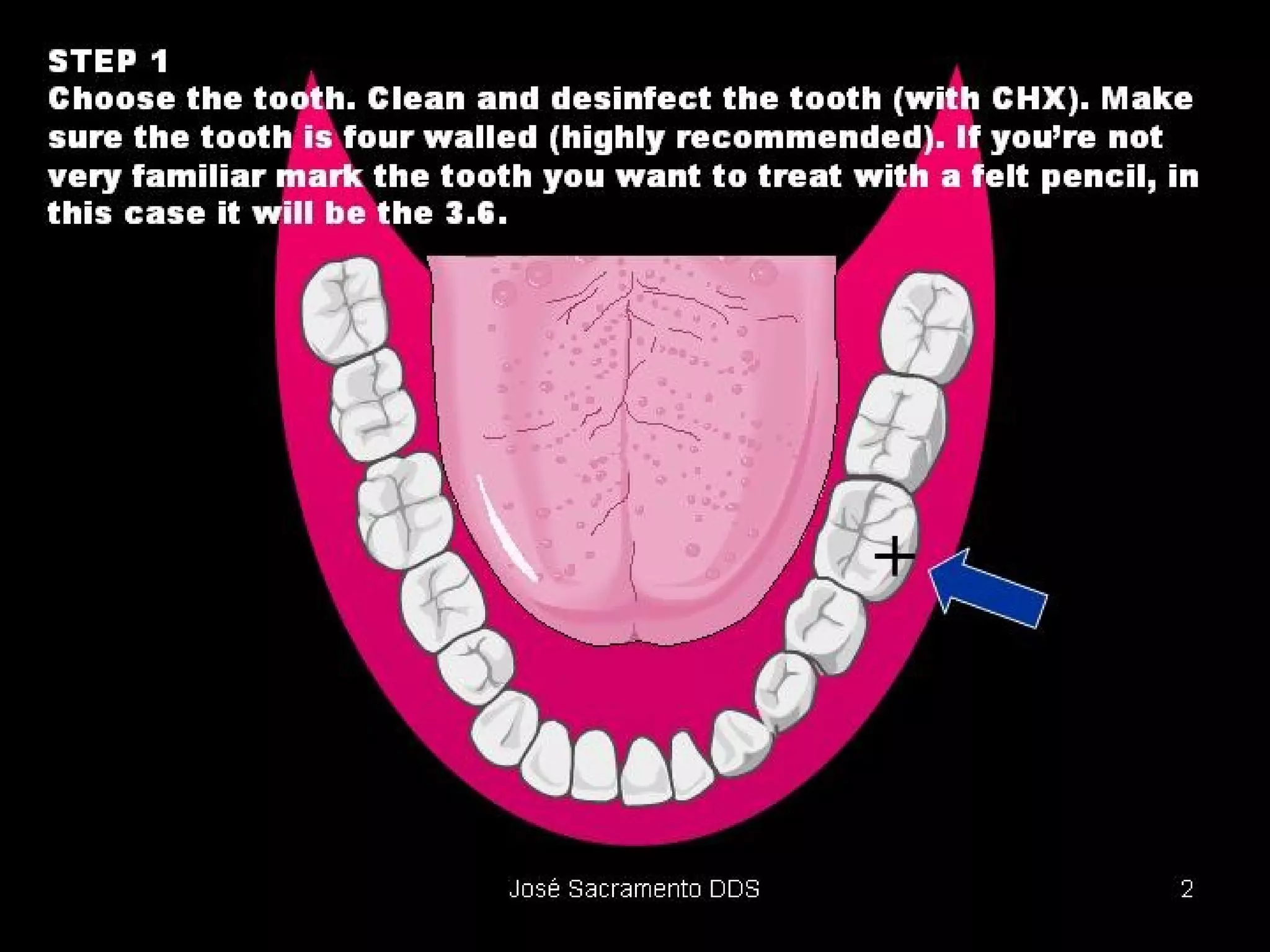
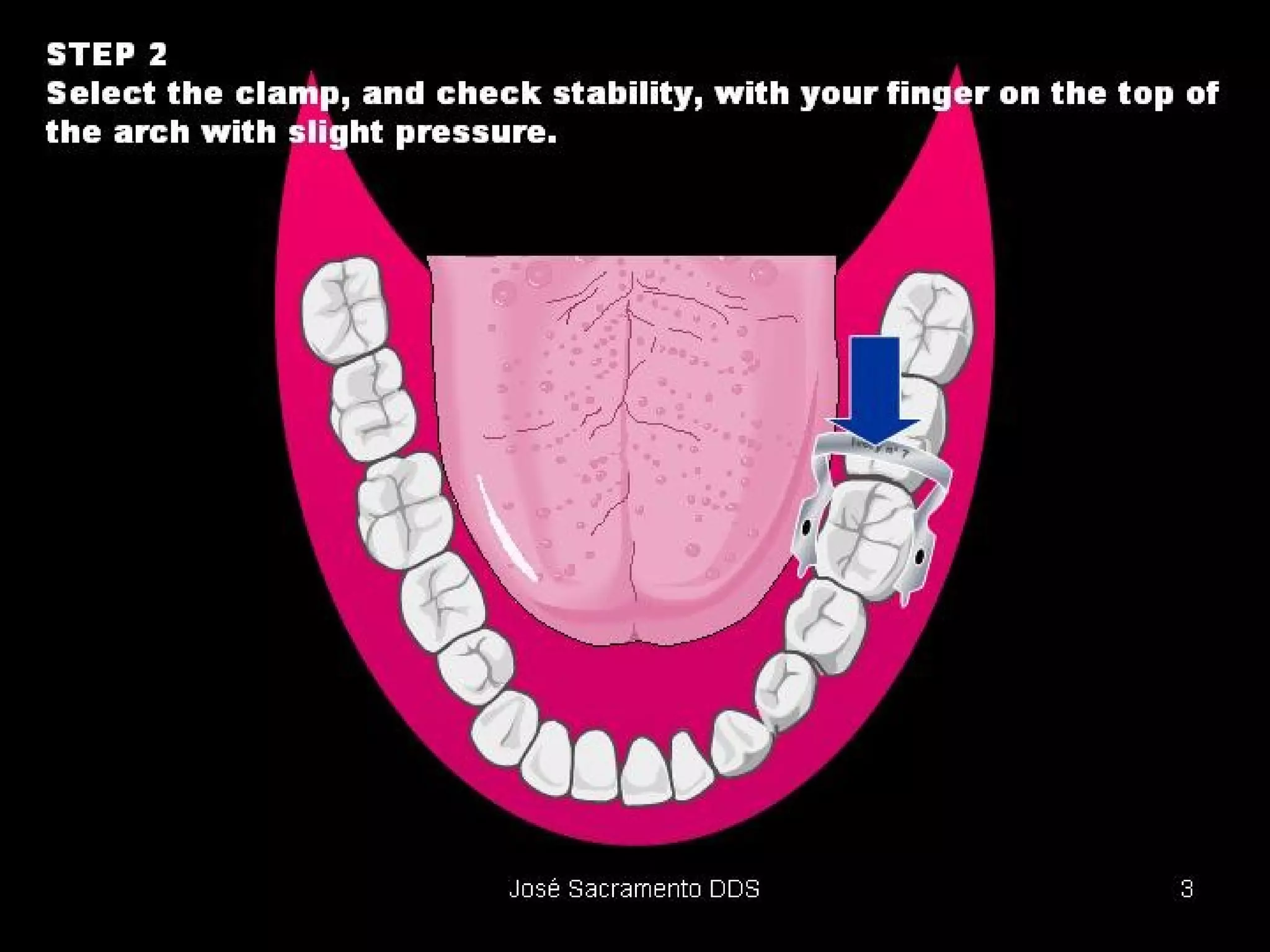
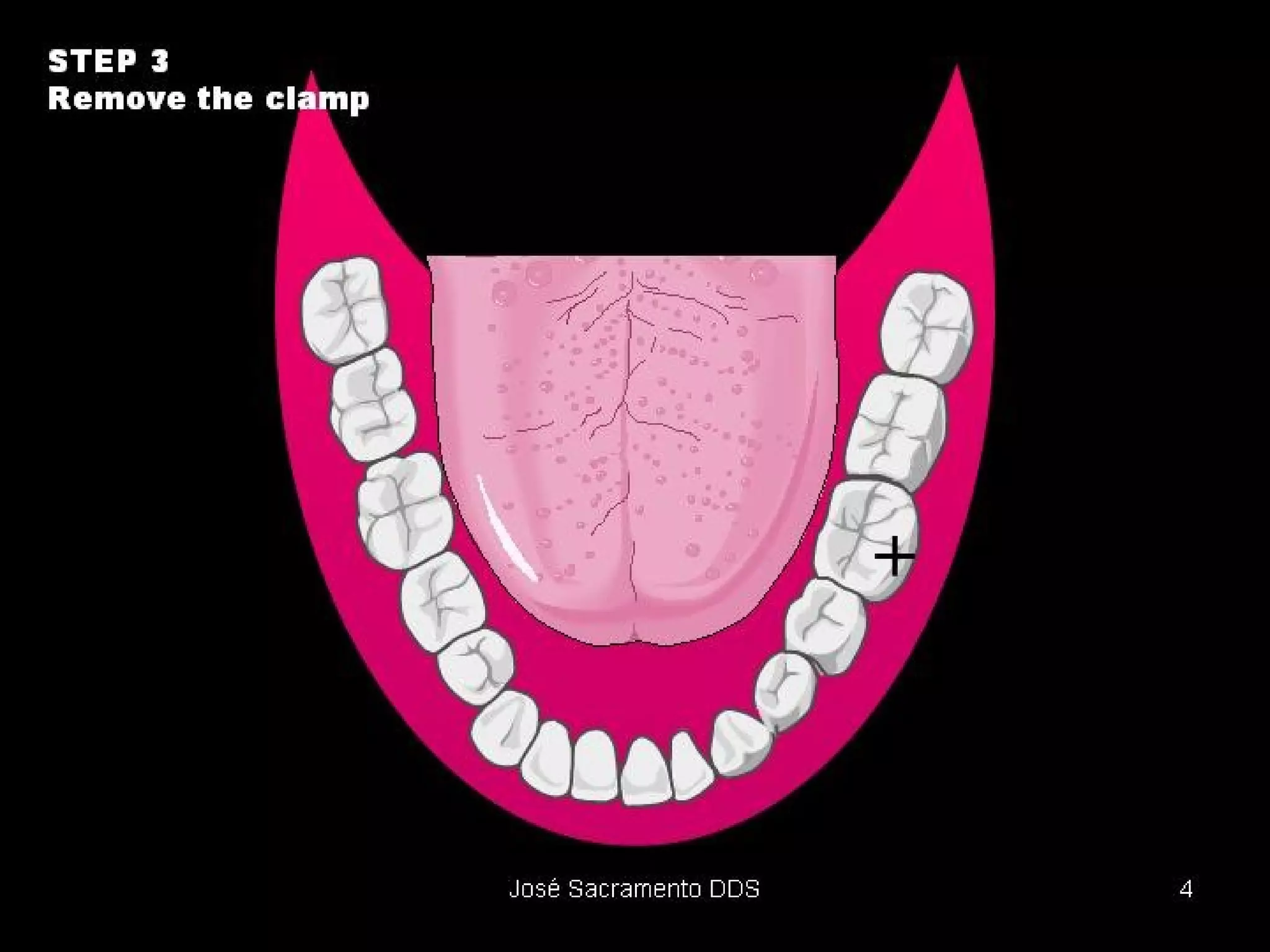
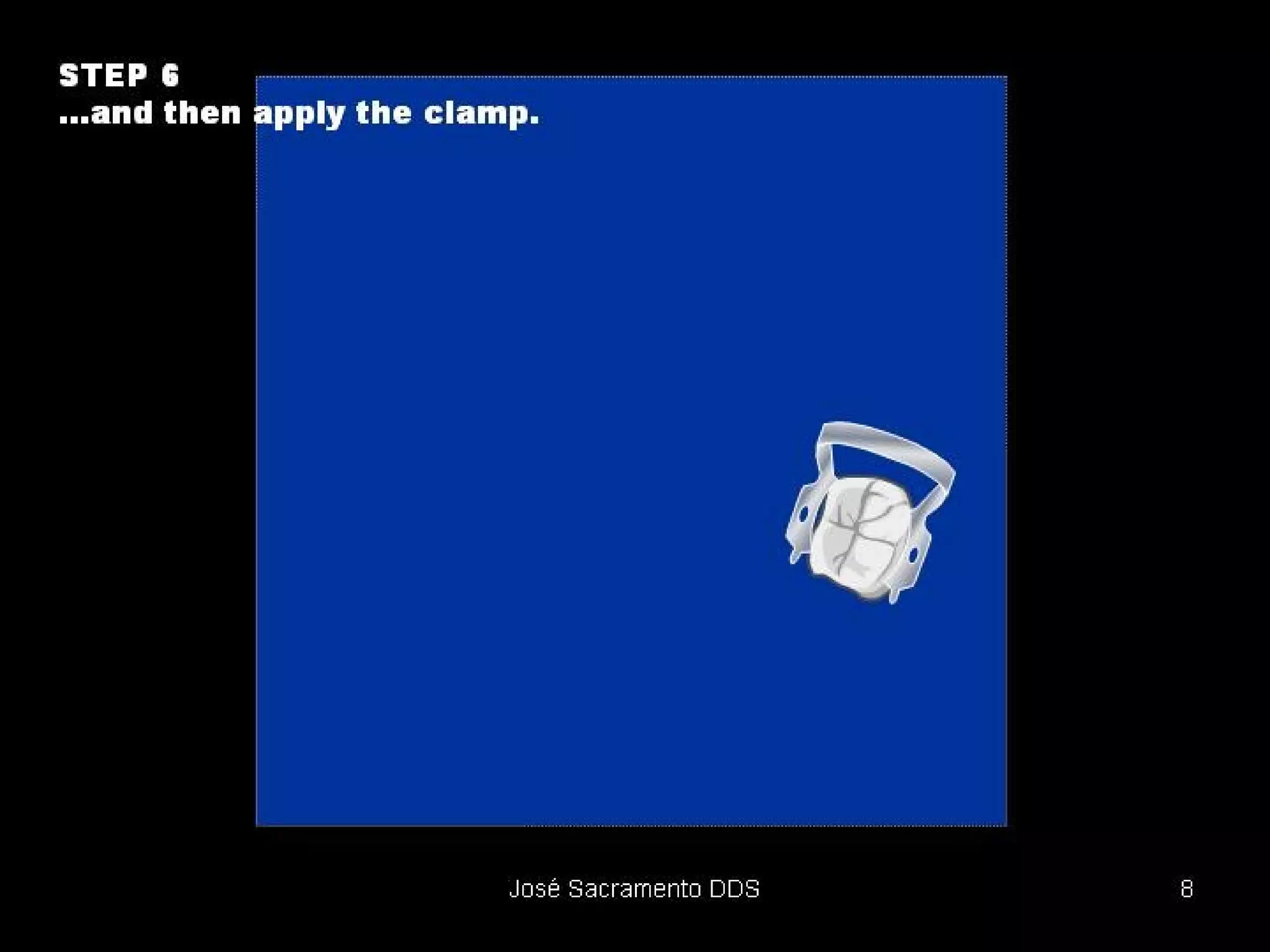
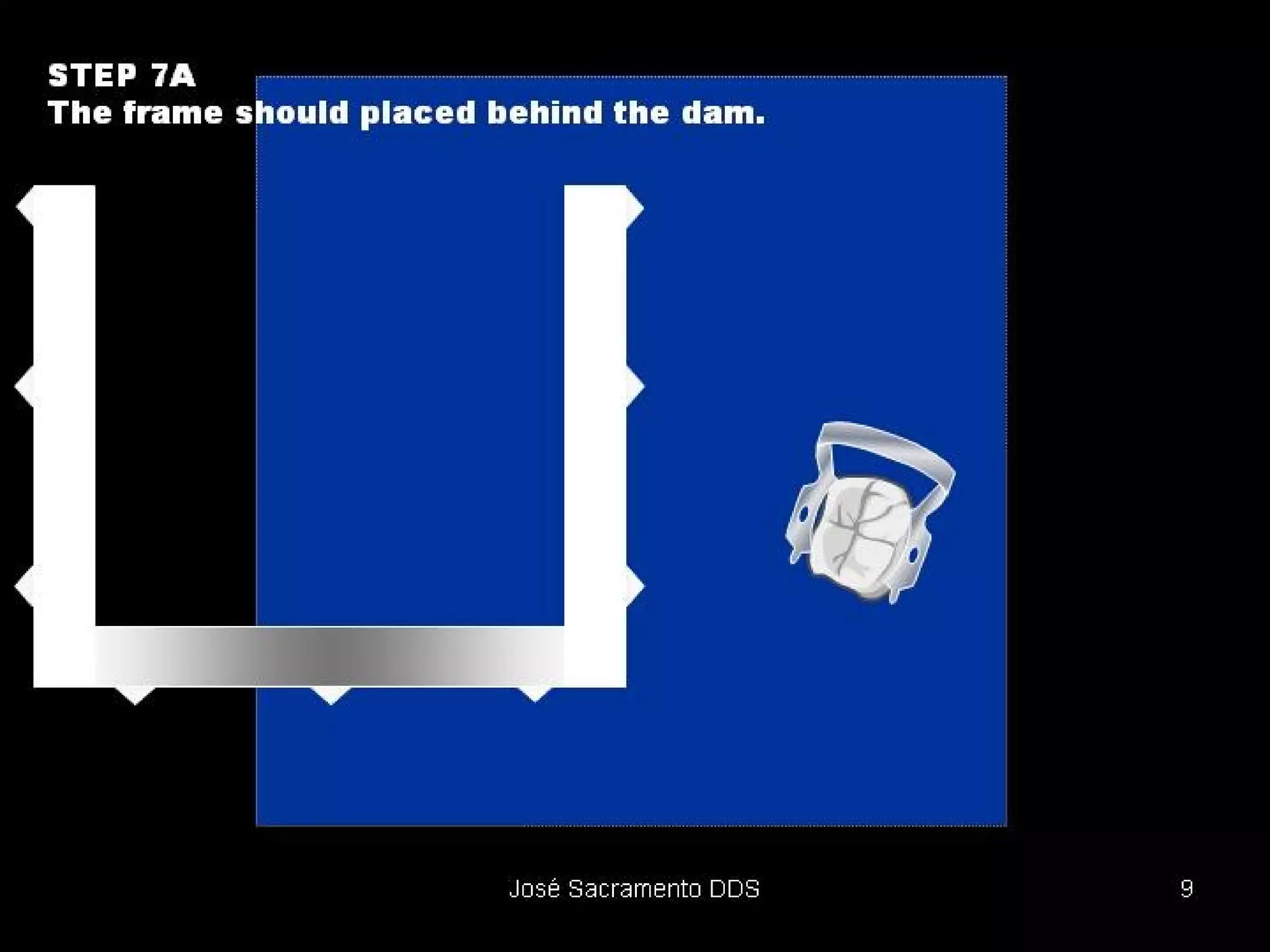
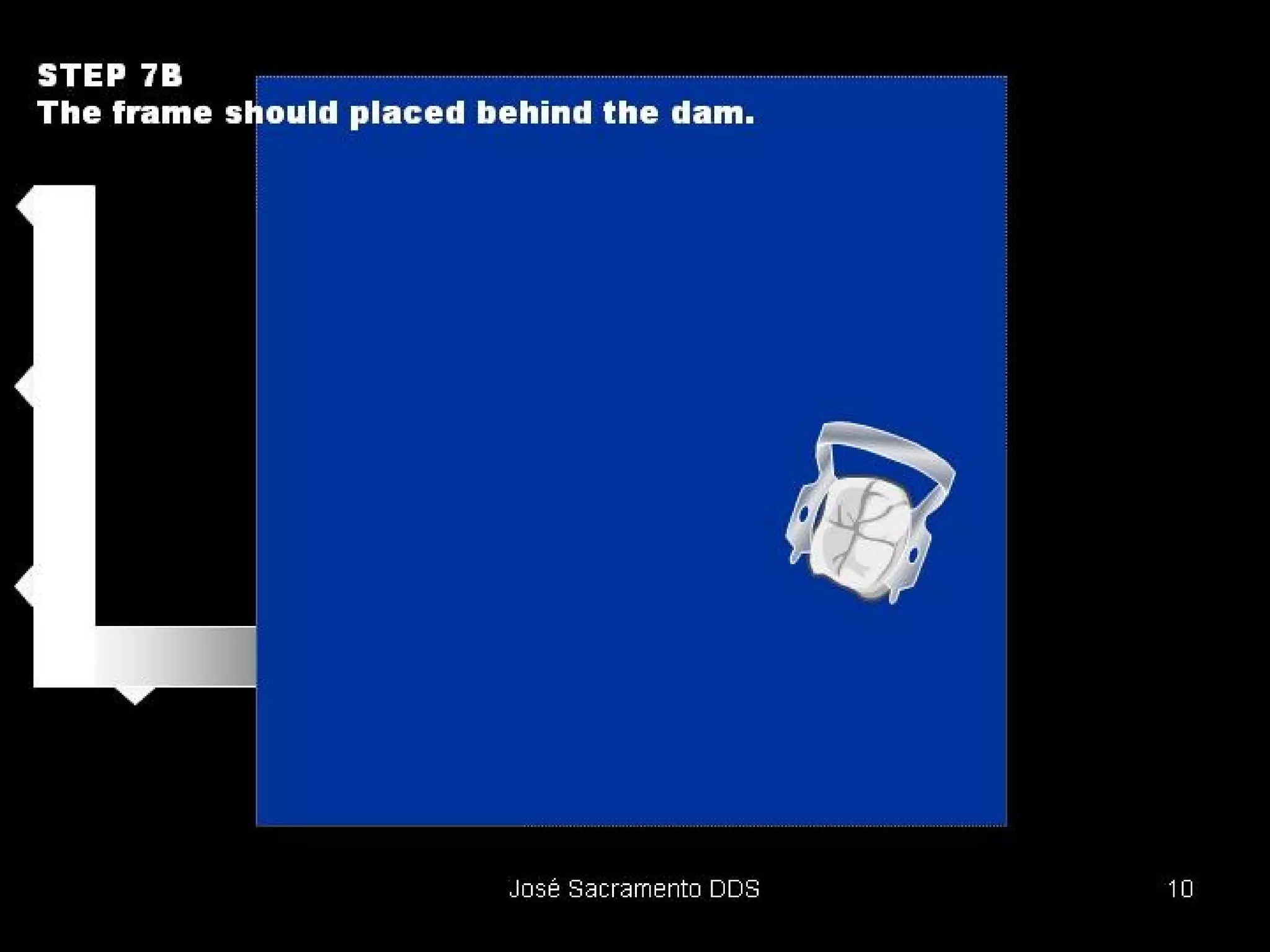
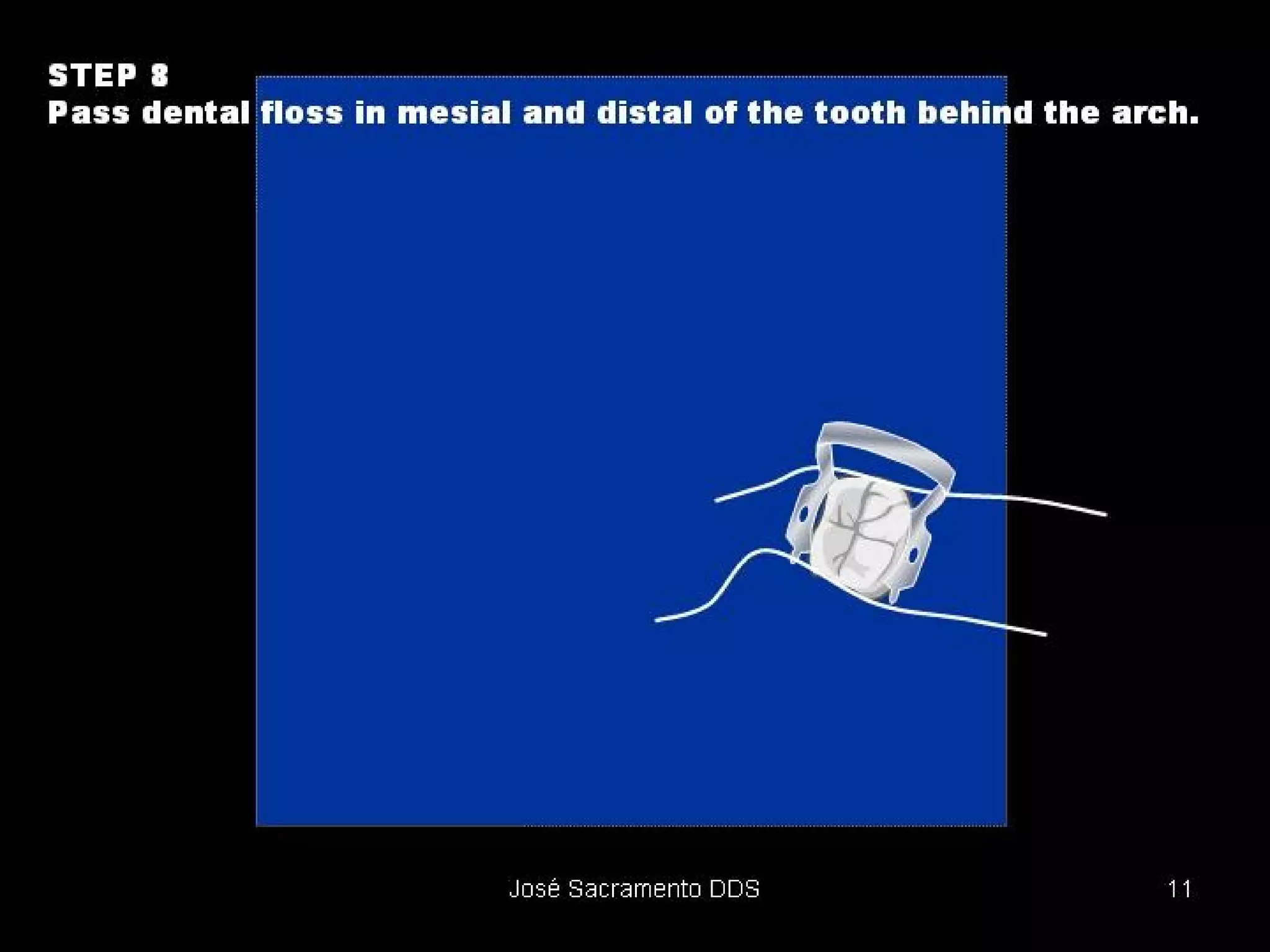
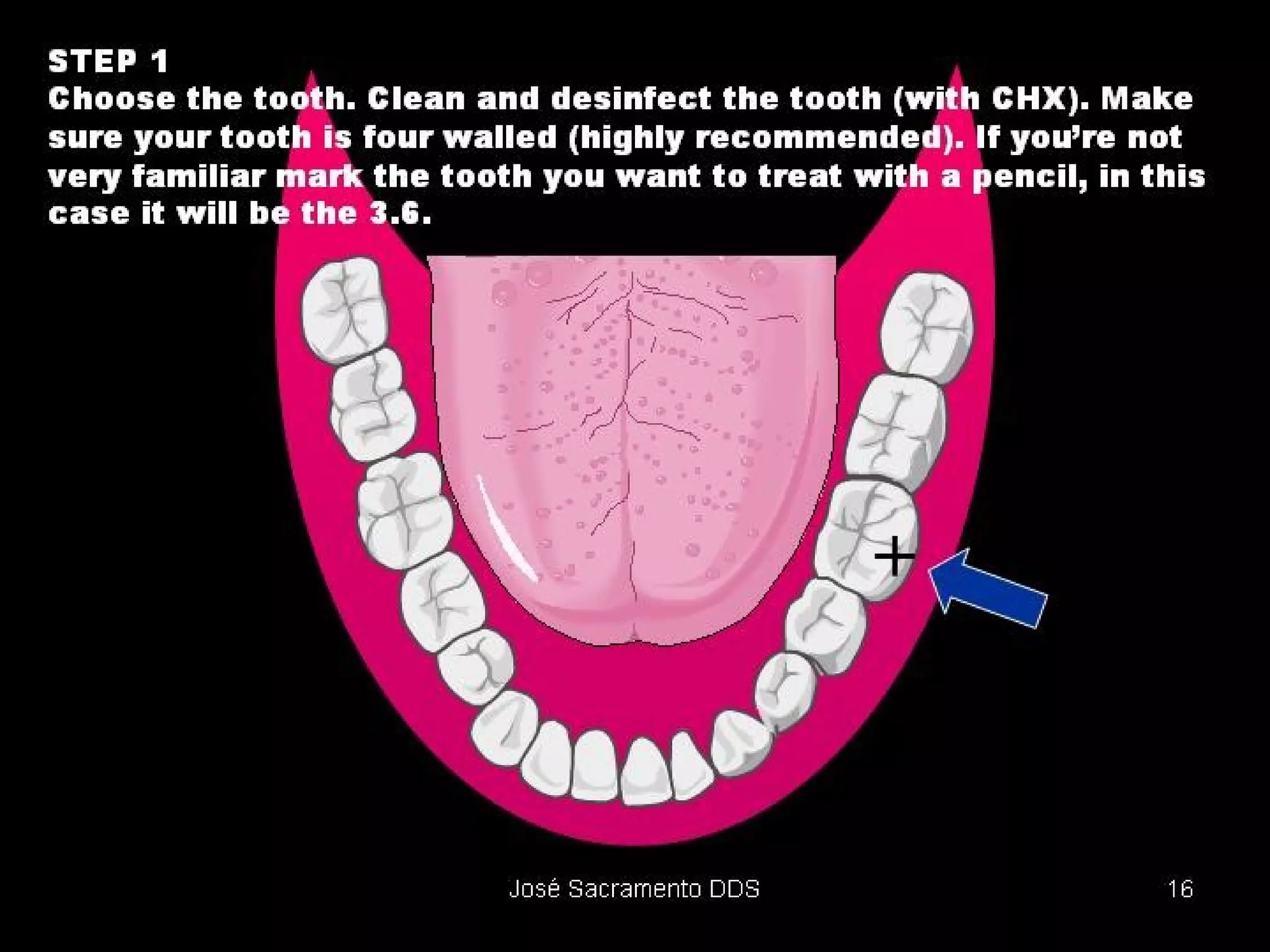
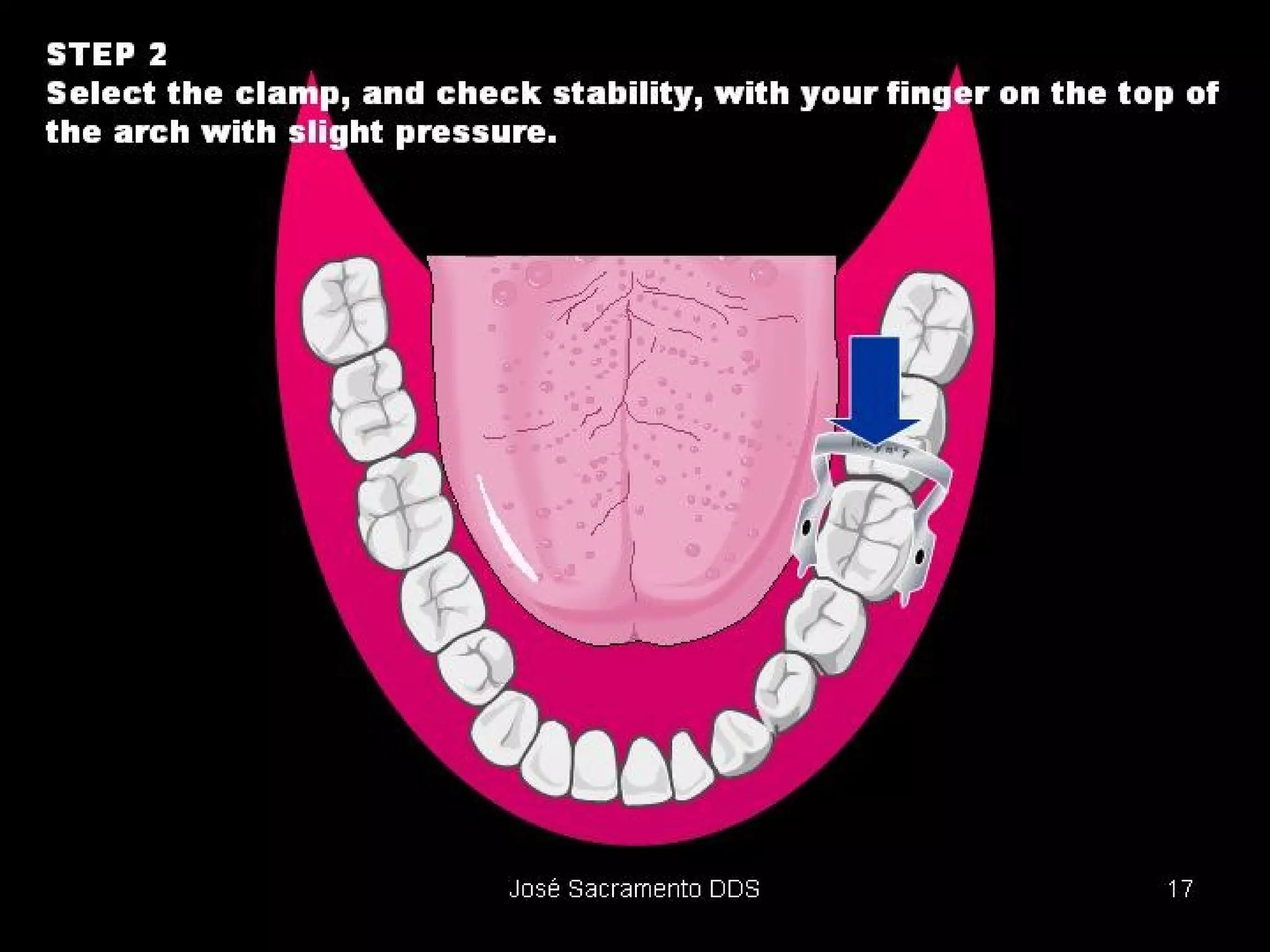
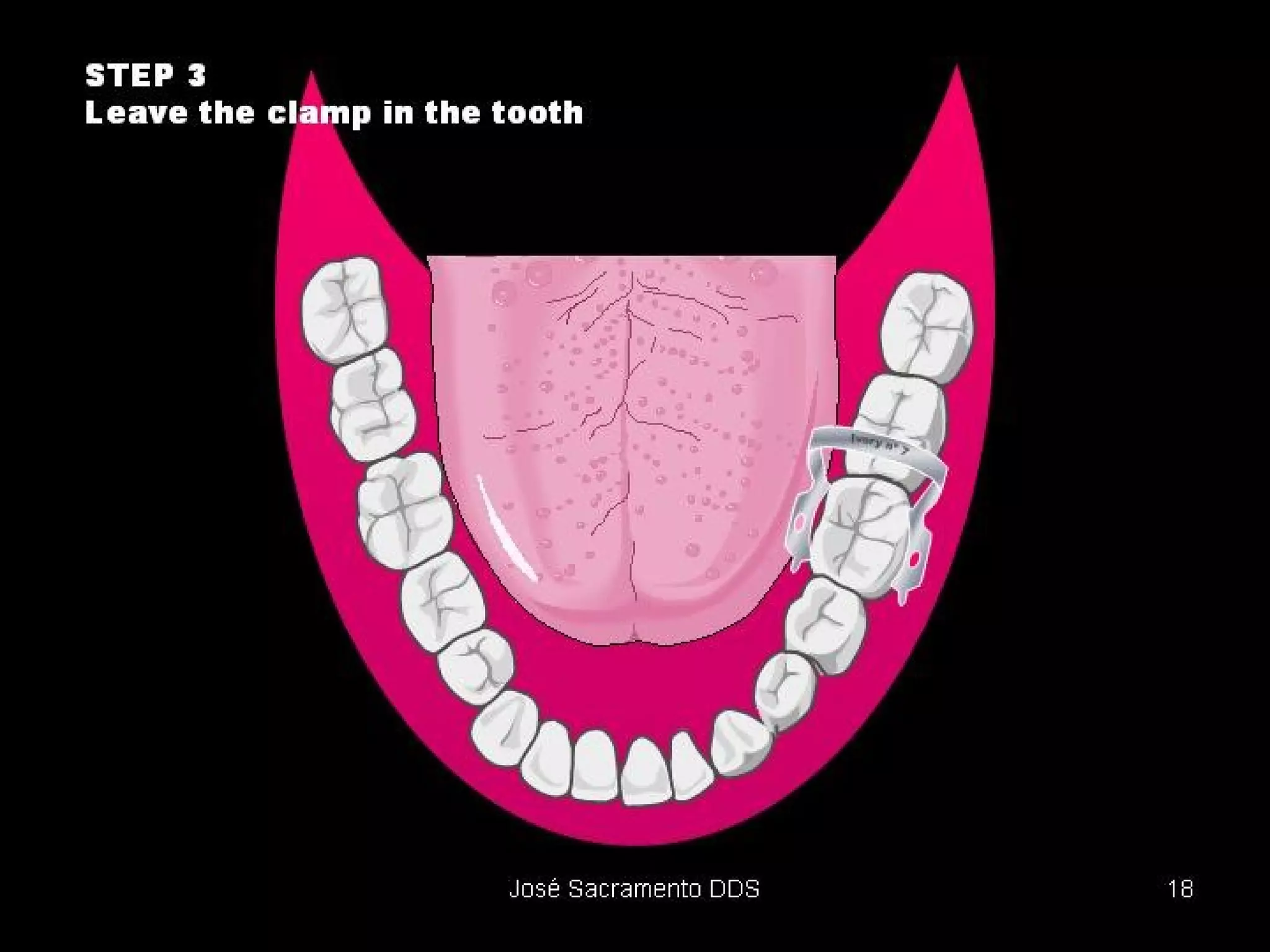
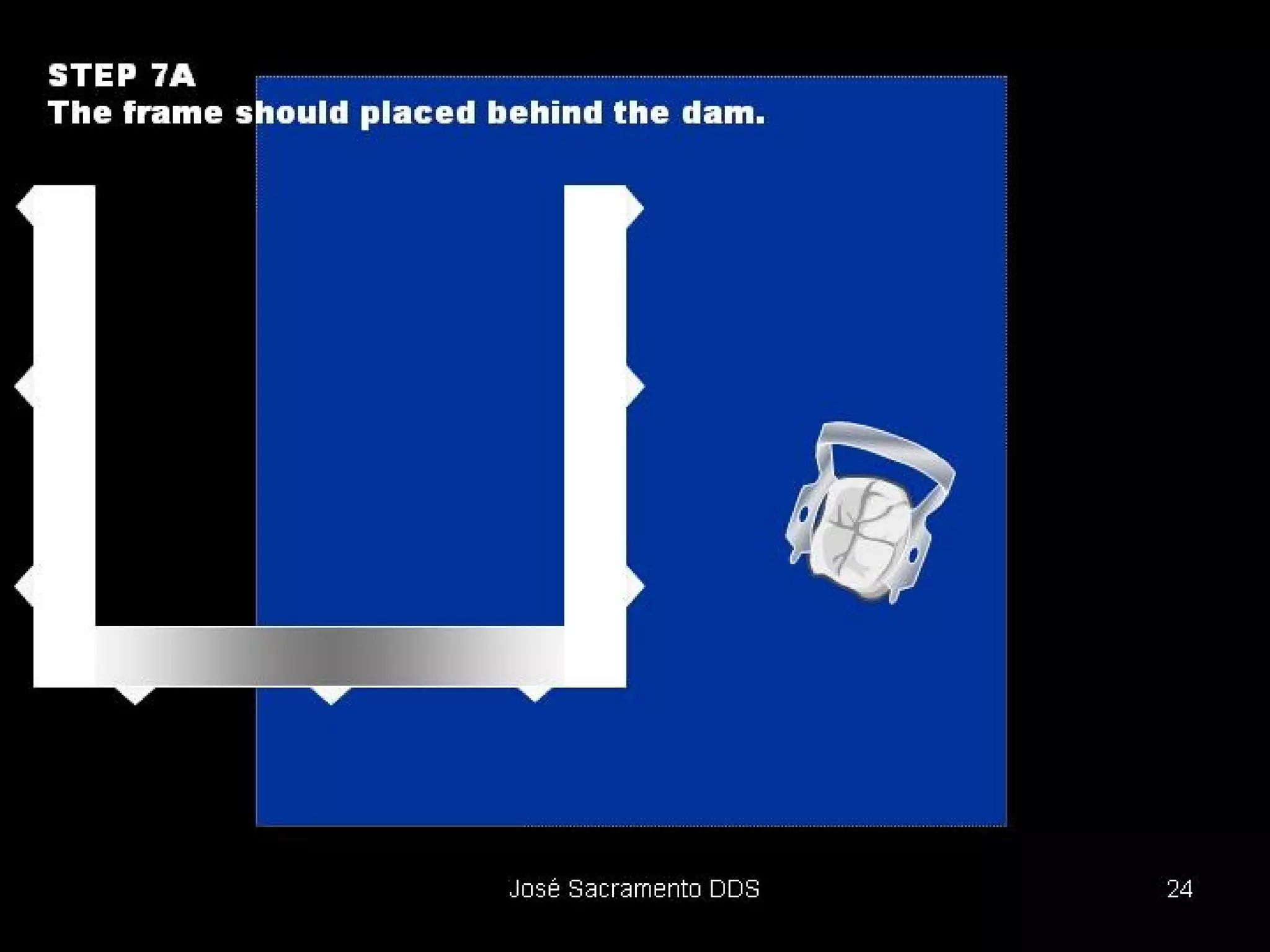
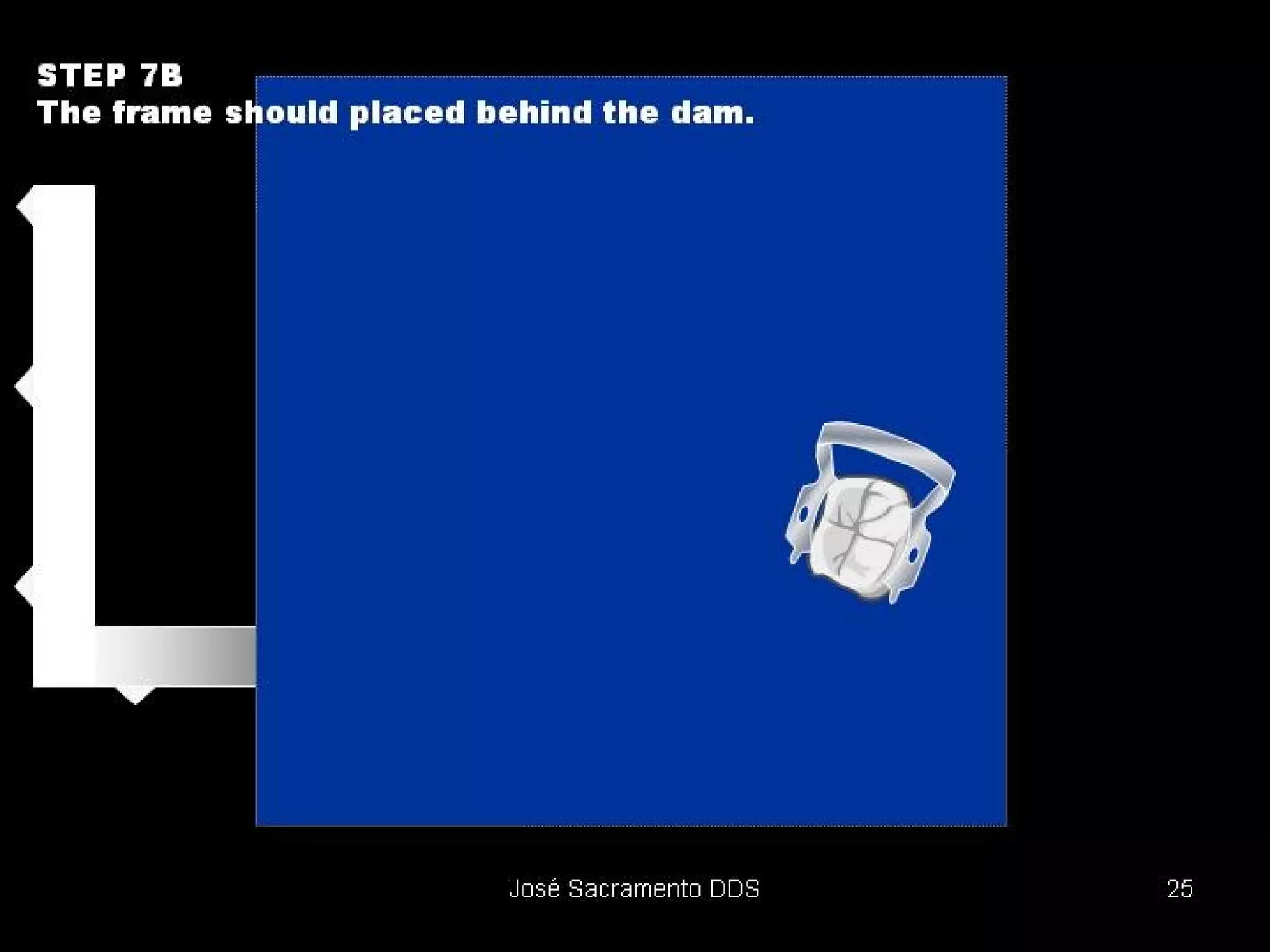
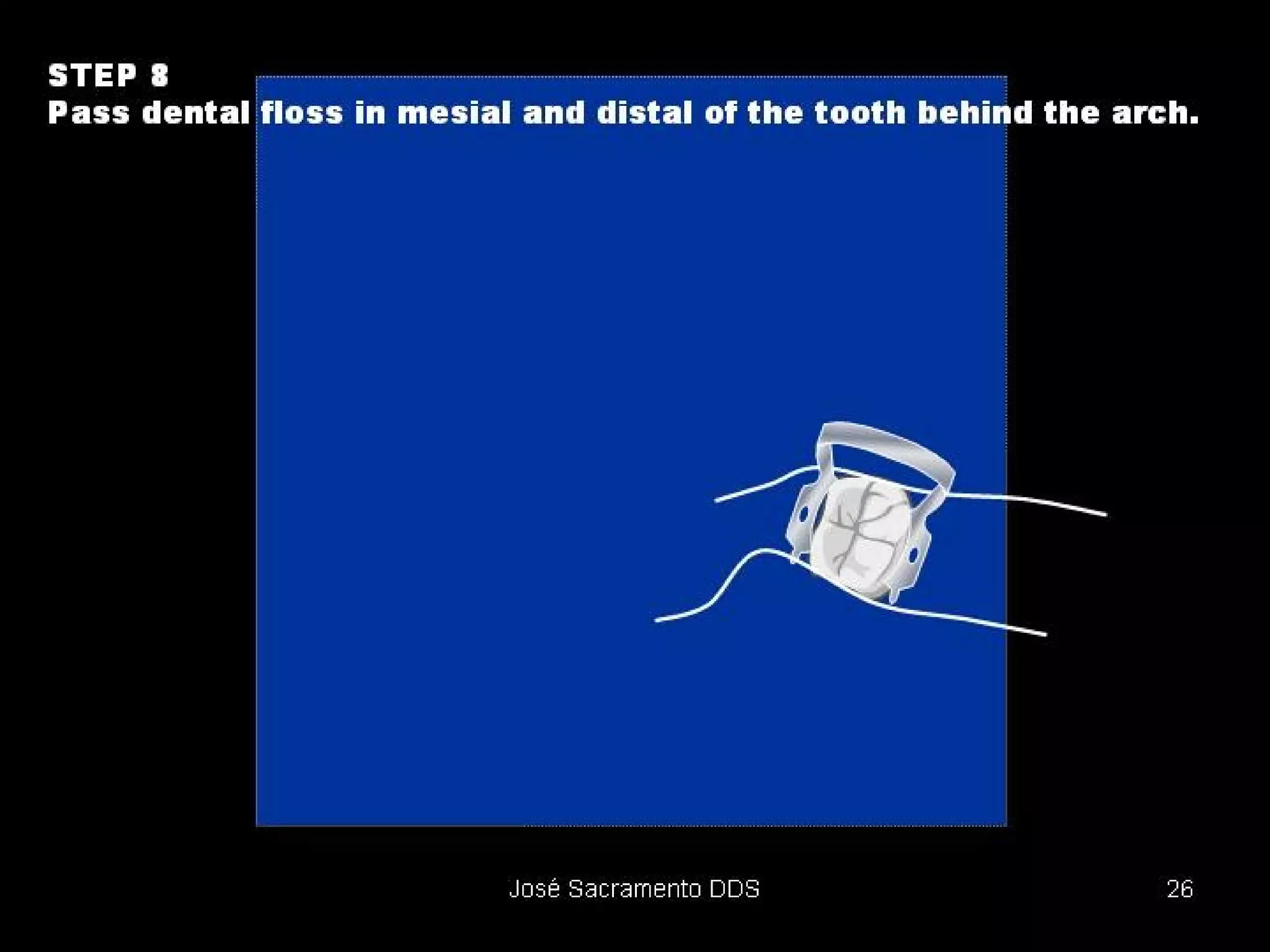
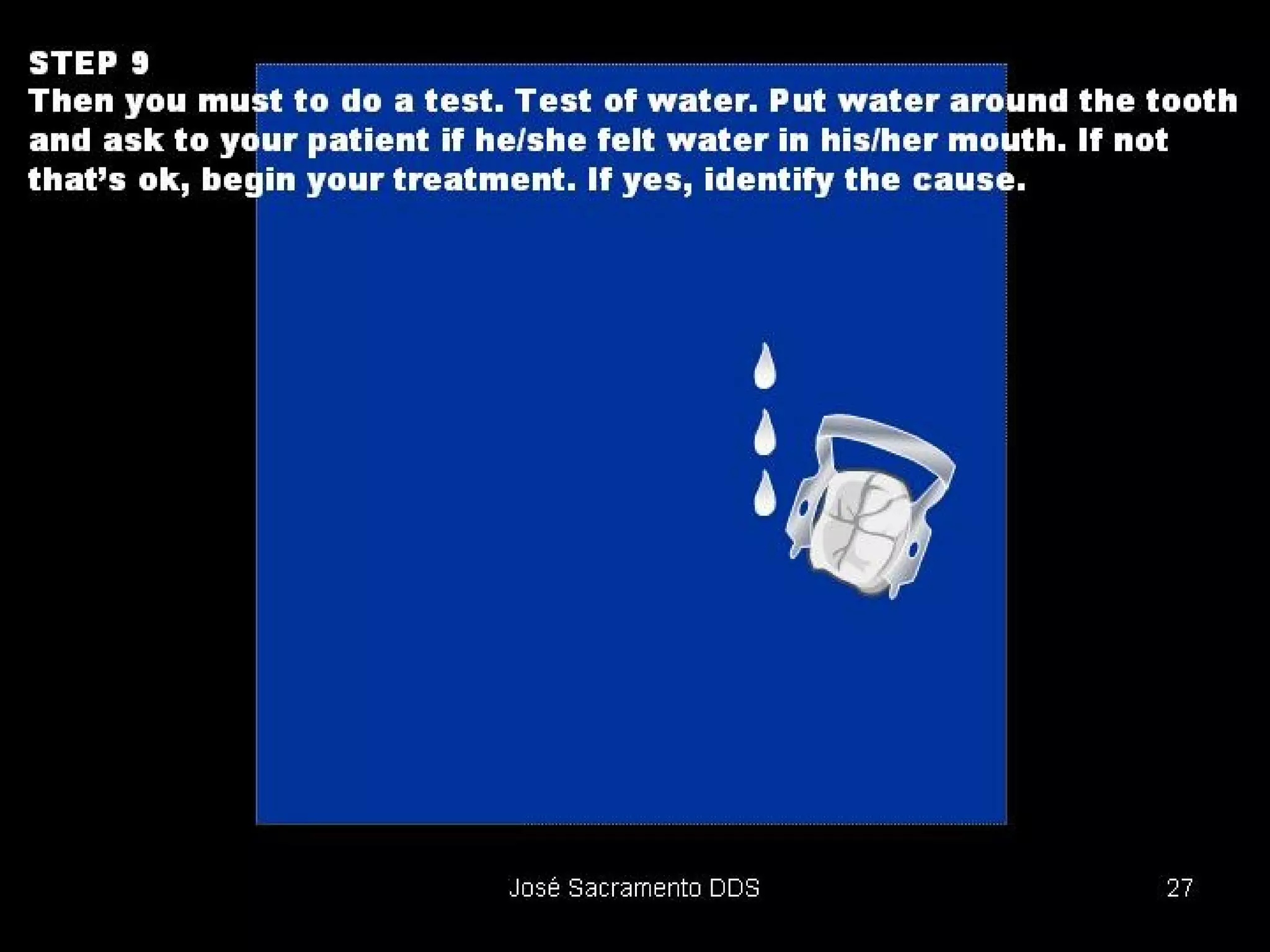
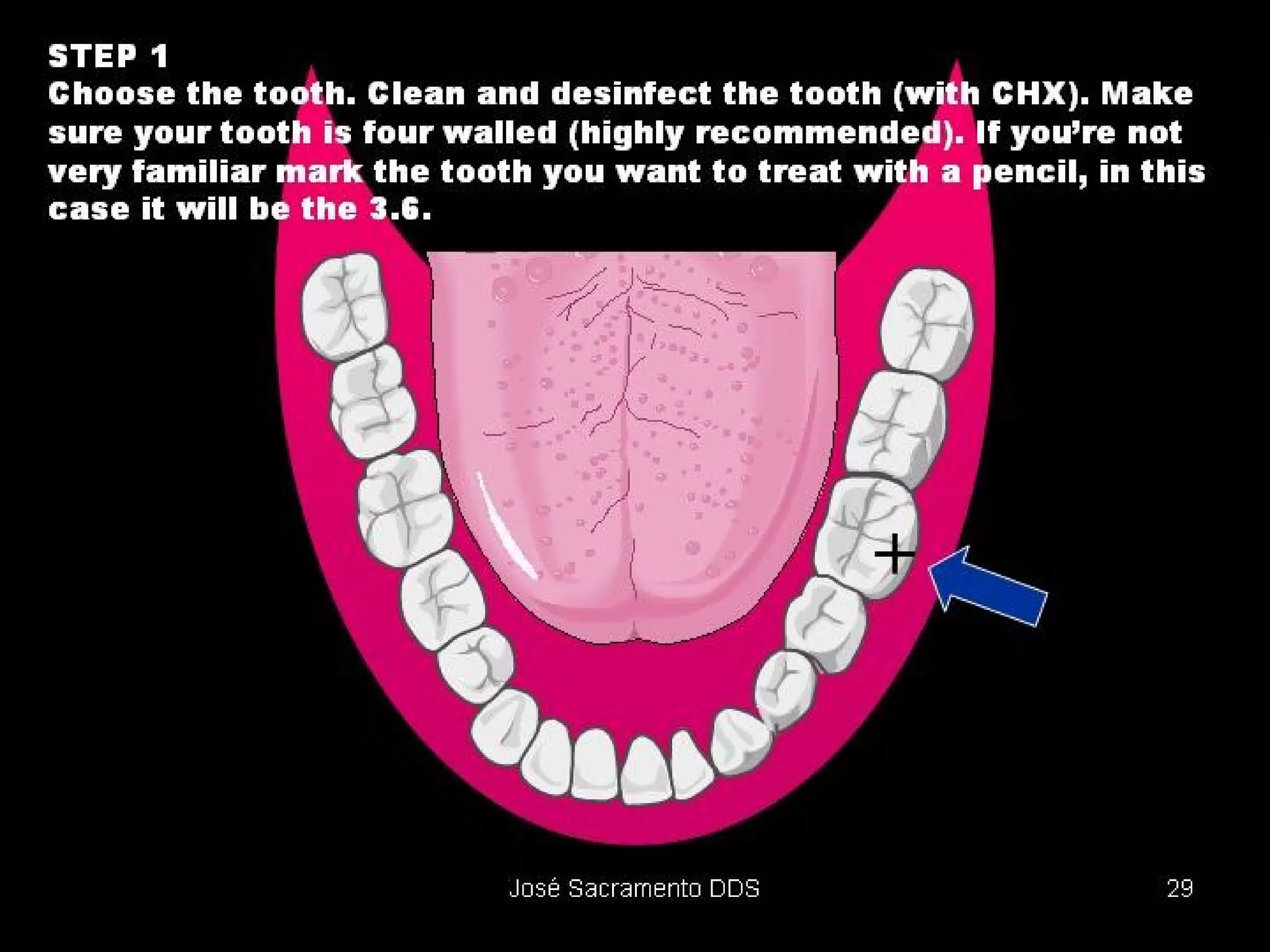
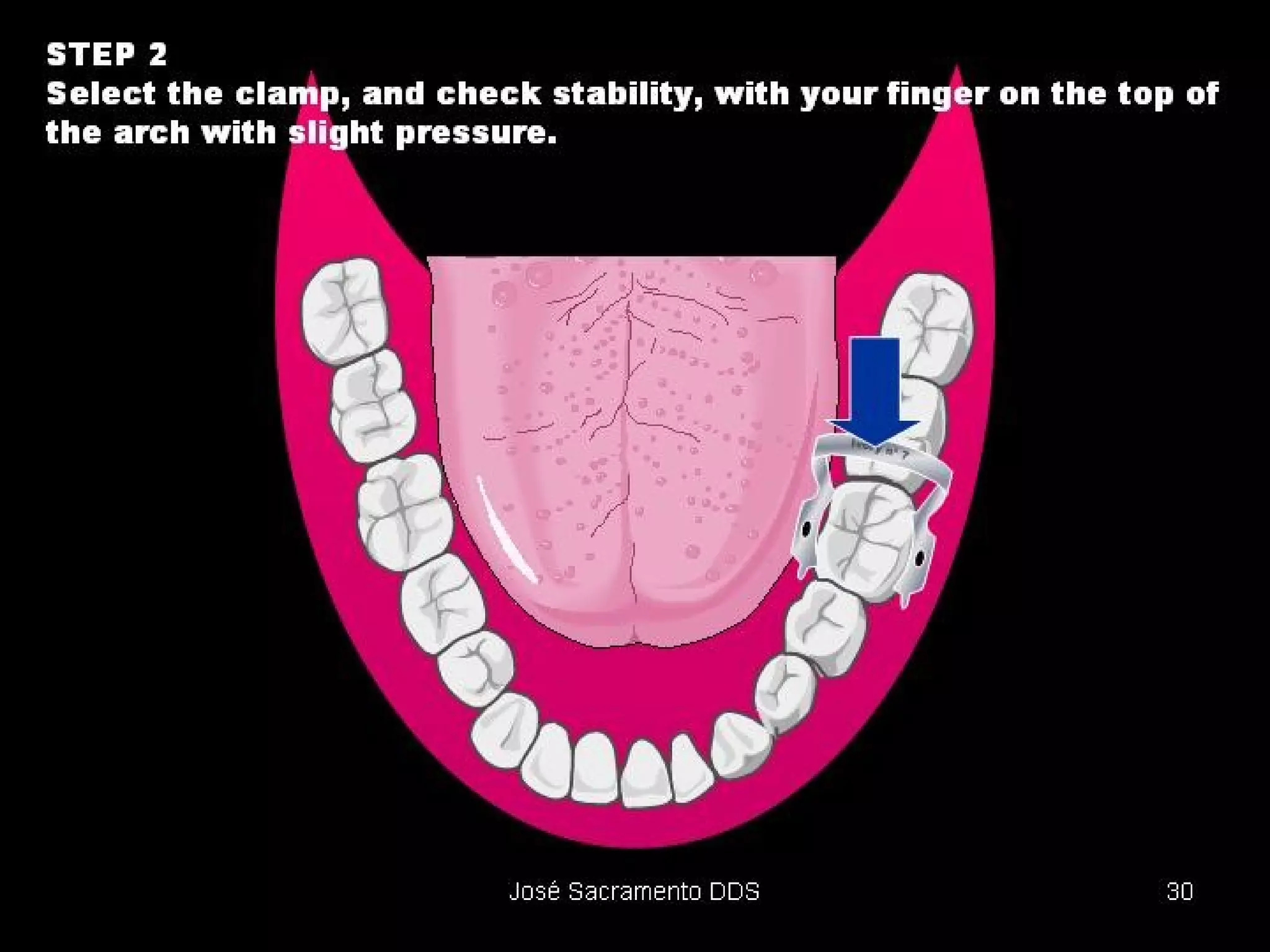
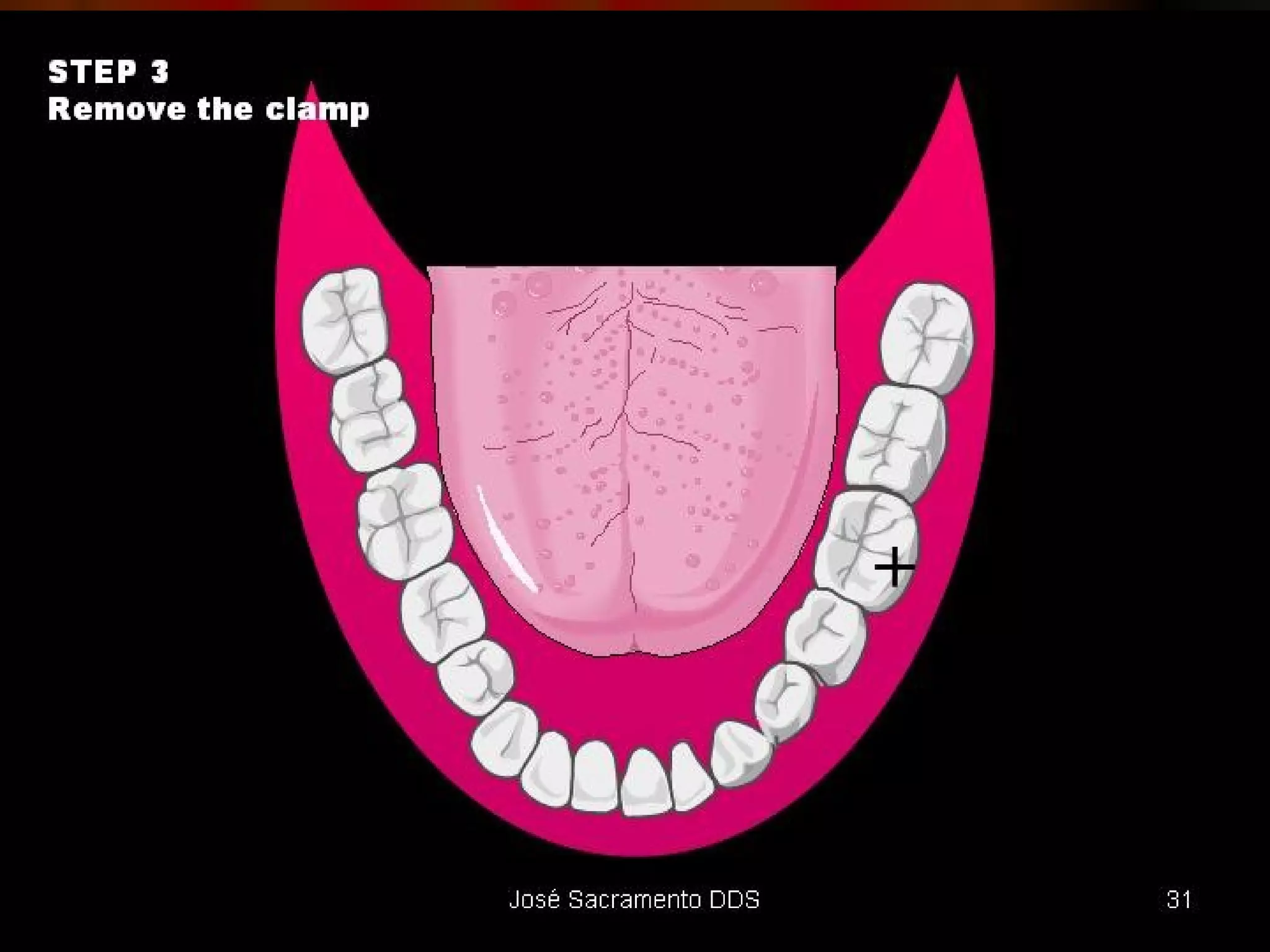
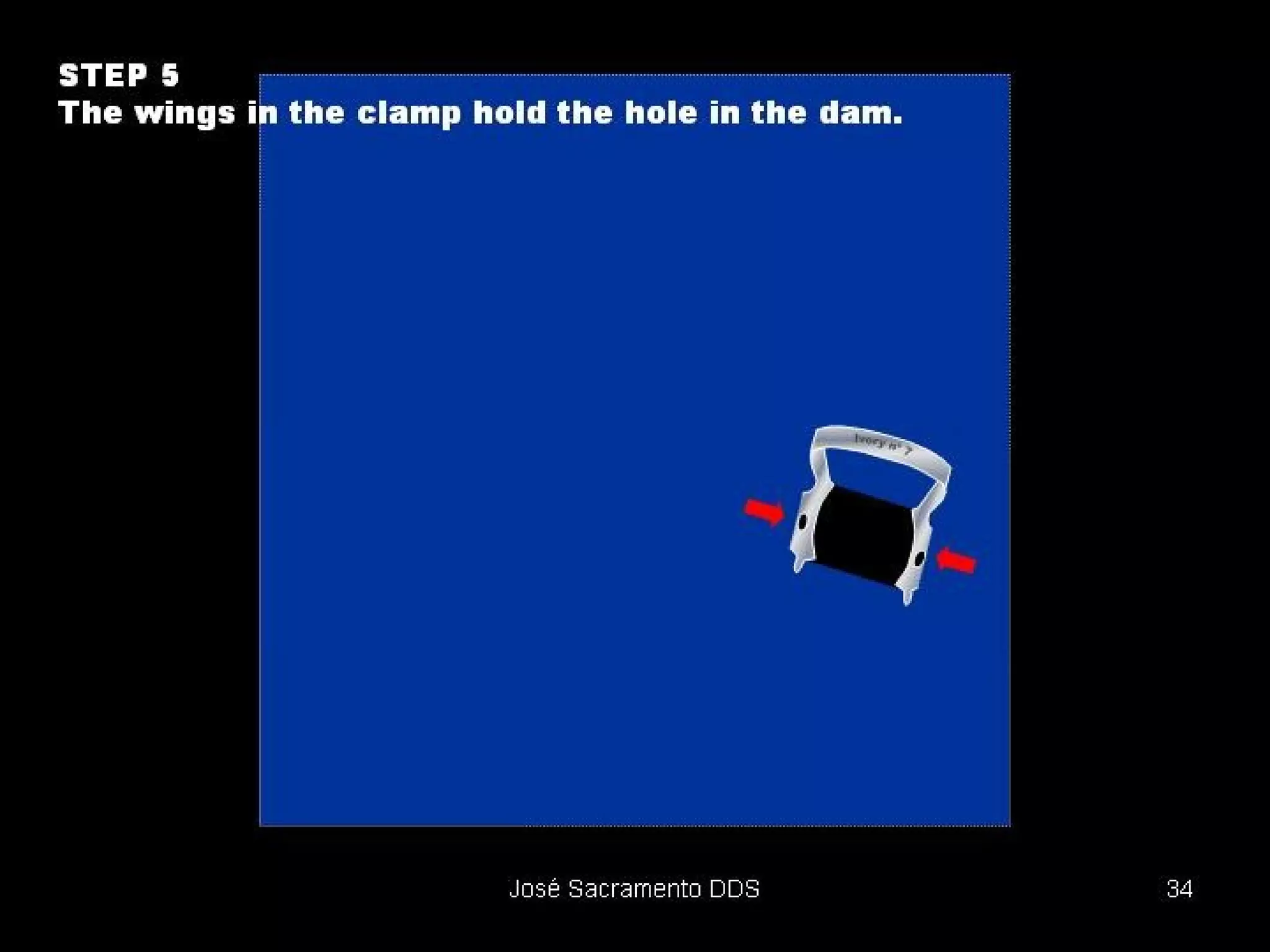
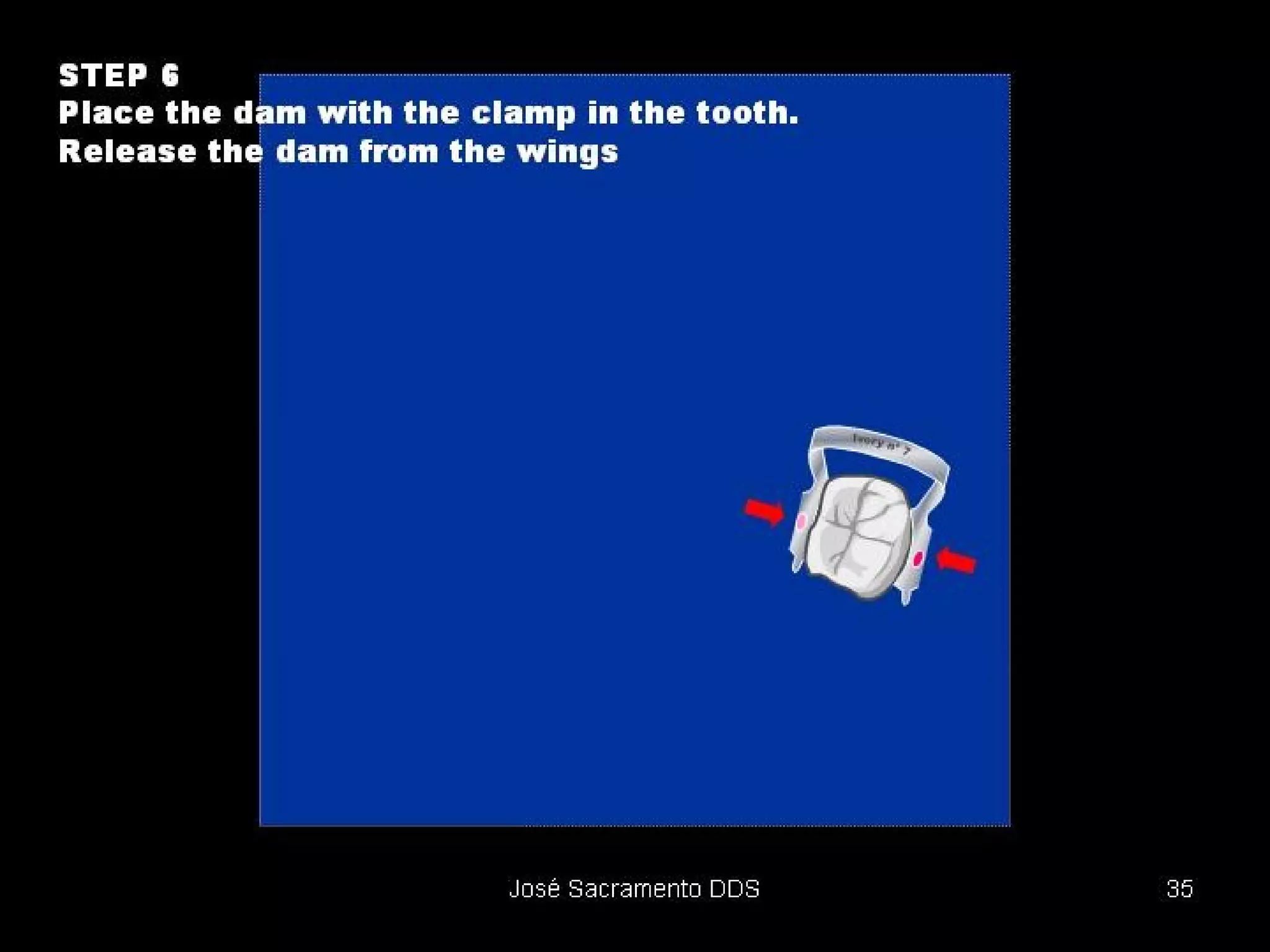
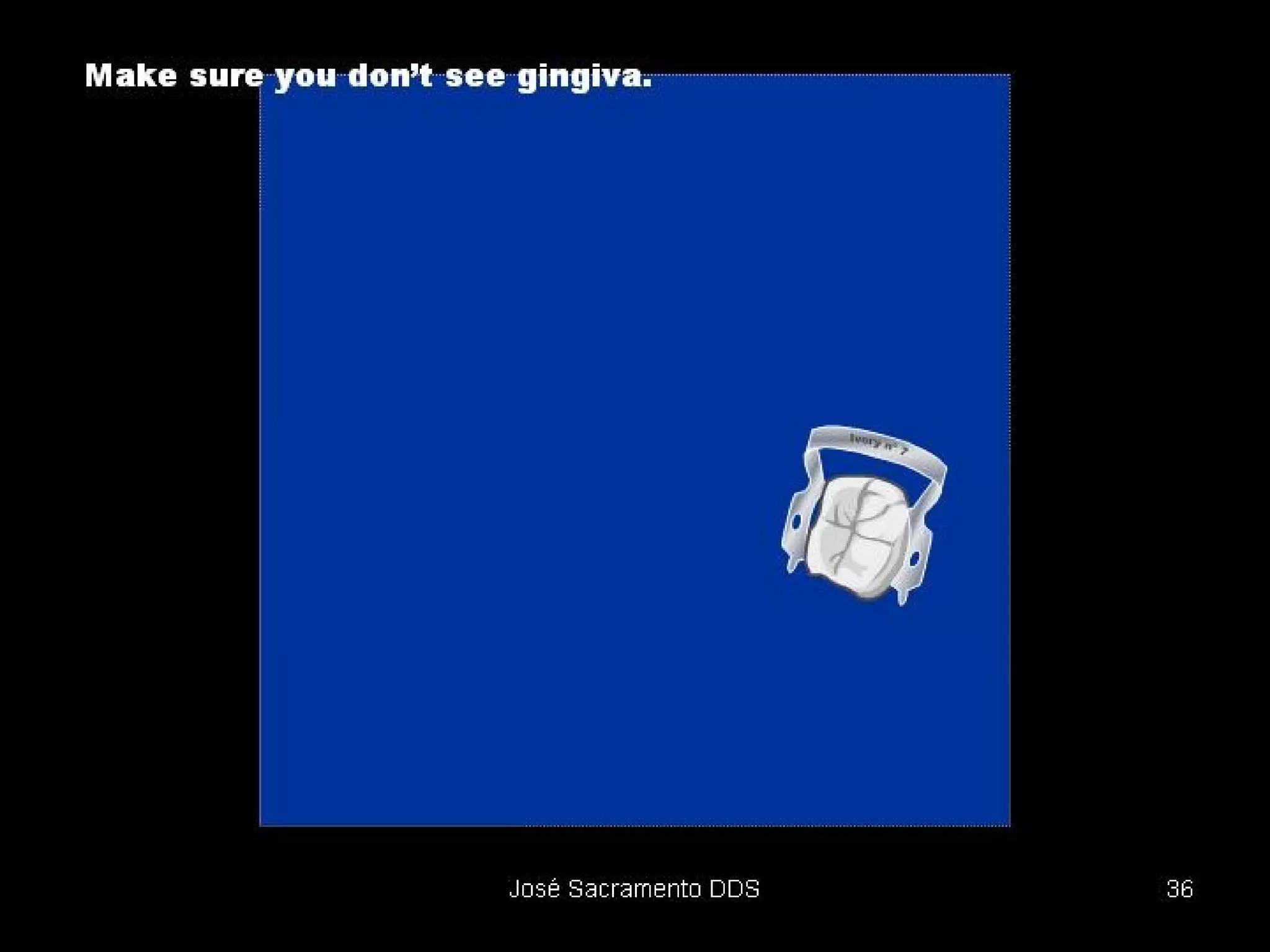
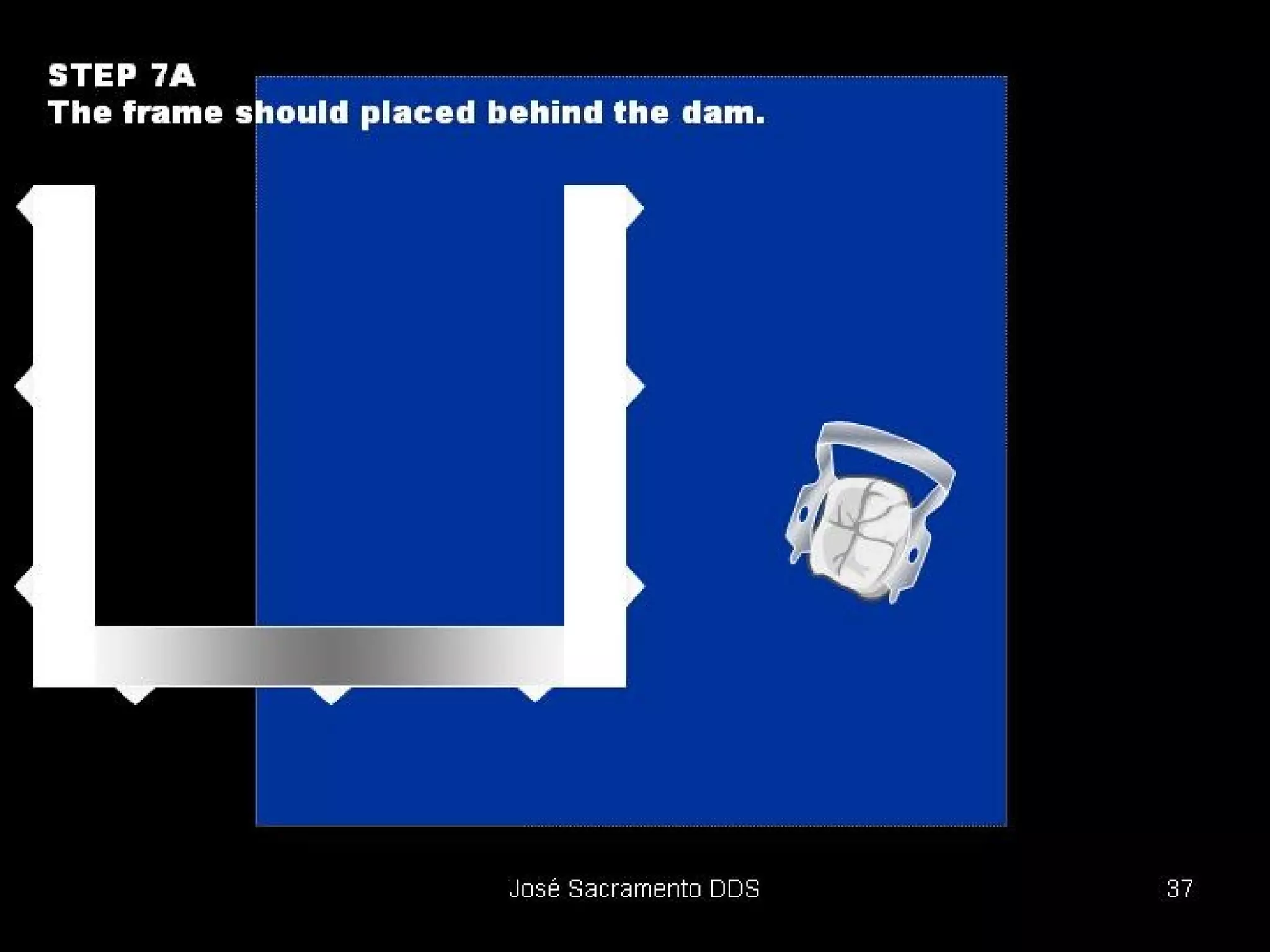
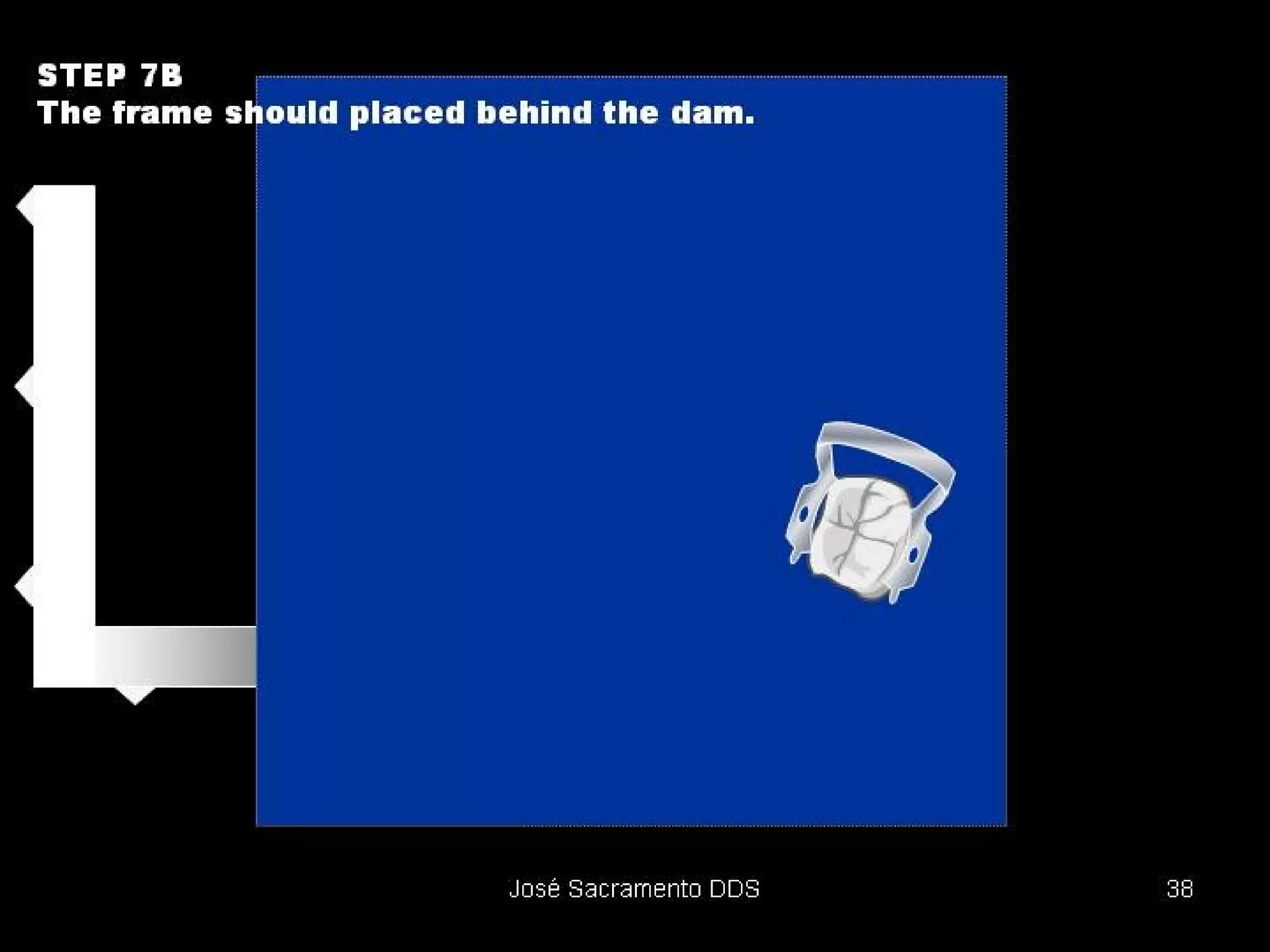
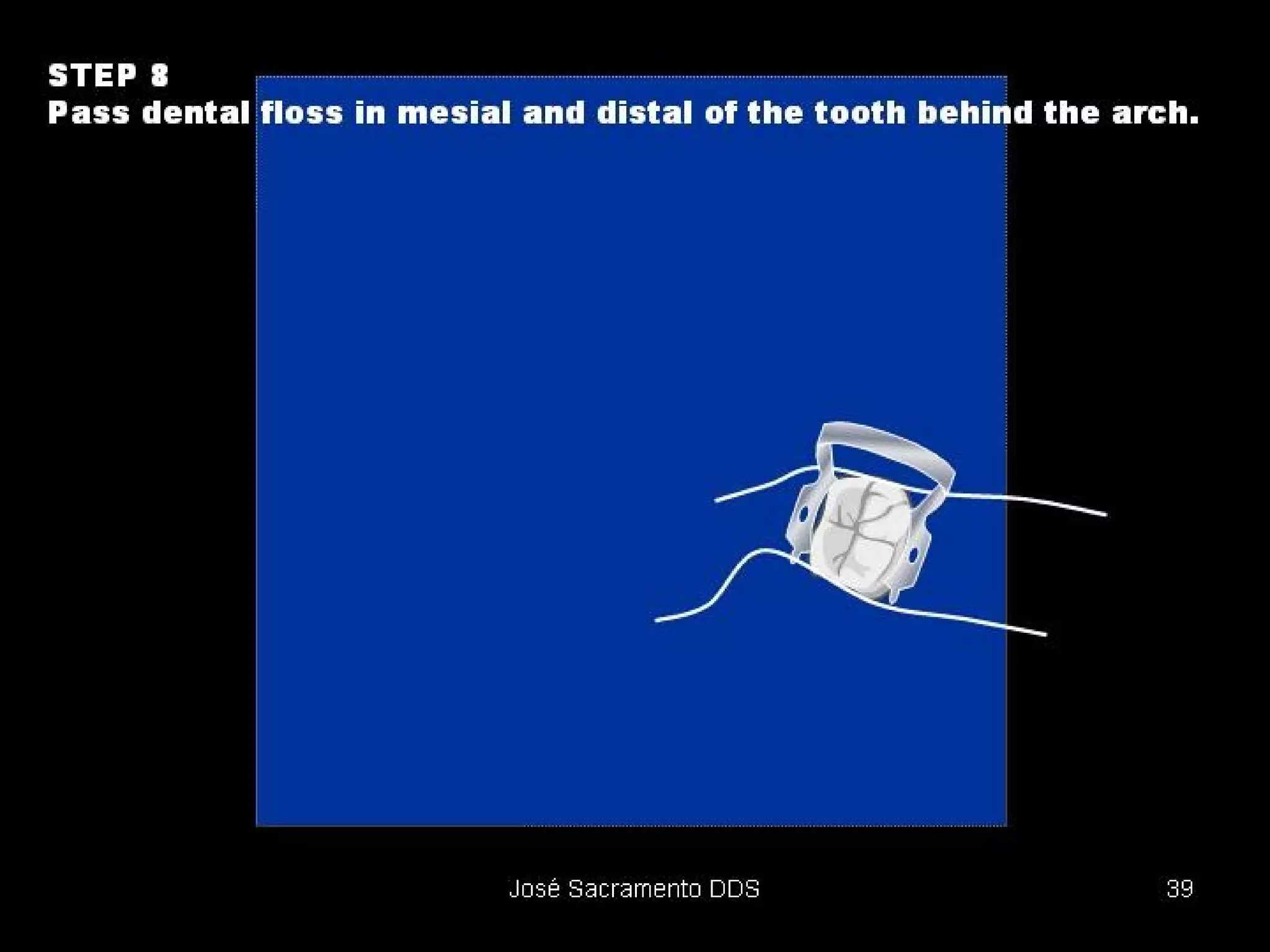







The document discusses the use of rubber dams in dentistry. It describes how rubber dams isolate the operating field, improve visibility and access, and prevent contamination. Key methods include using a rubber dam sheet held in place by a clamp on the tooth with a hole for access. Advantages include isolation, improved properties of materials, and protection of the patient. Placement involves several steps and materials like clamps, frames, and punches.














































![Isolation-of-the-operating-field[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/isolation-of-the-operating-field1autosaved-250226051150-dcc1b95b-thumbnail.jpg?width=640&height=640&fit=bounds)








































