Downloaded 10 times


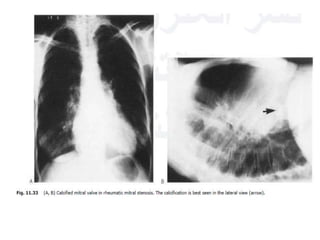
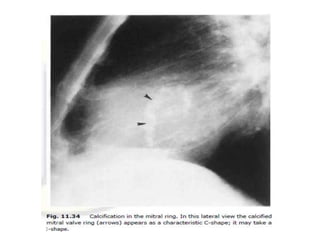

This document summarizes various heart diseases including coronary heart disease, stable angina, acute myocardial infarction, valvular heart diseases, and their appearances on chest radiographs. Coronary artery disease is caused by atherosclerosis and presents as coronary calcification or cardiomyopathy. Acute MI can cause pulmonary edema on CXR. Valvular diseases like aortic stenosis present with left ventricular hypertrophy and calcification while aortic regurgitation causes cardiomegaly. Mitral stenosis presents with left atrial enlargement and pulmonary hypertension.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

