Download to read offline












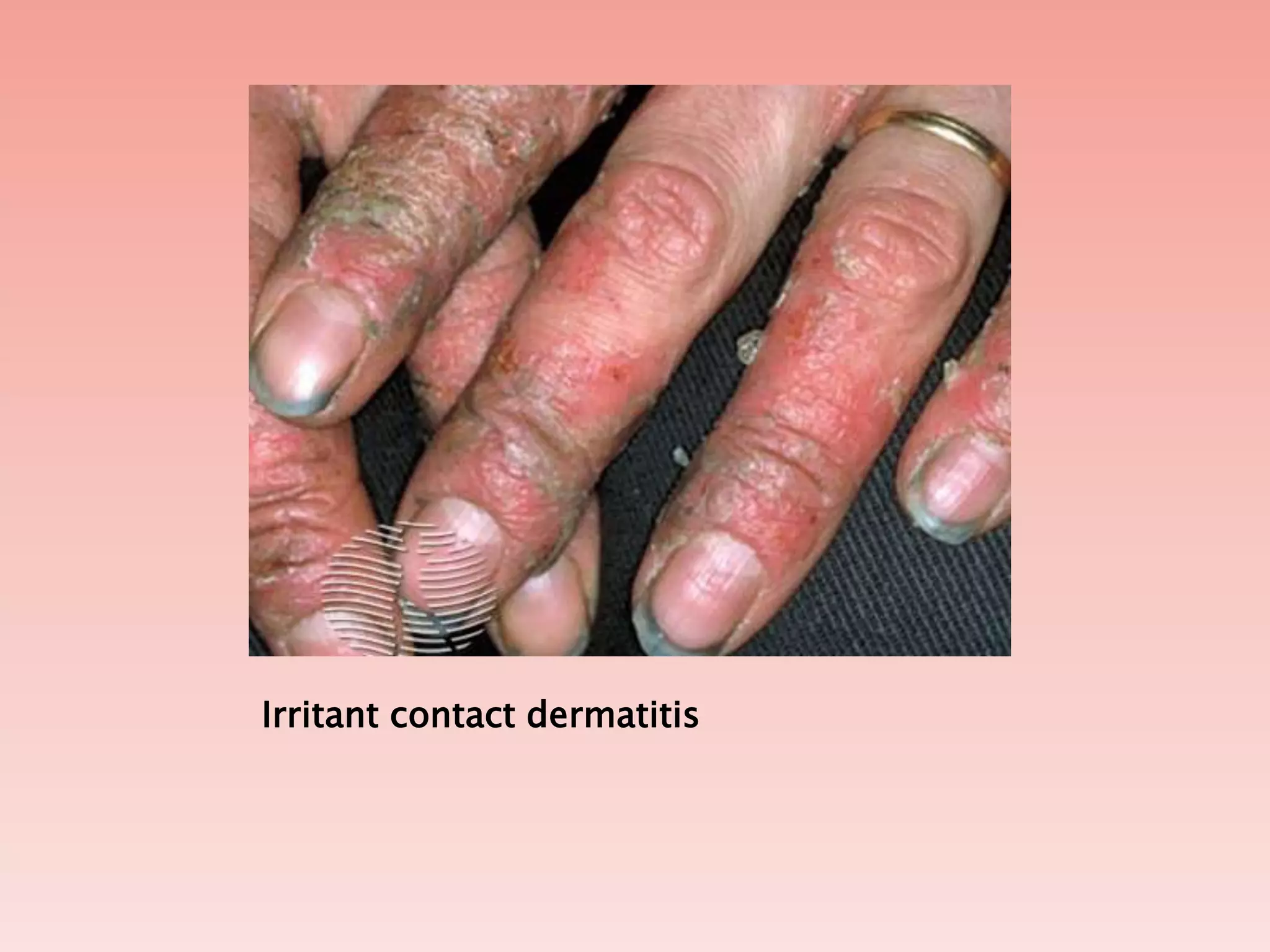
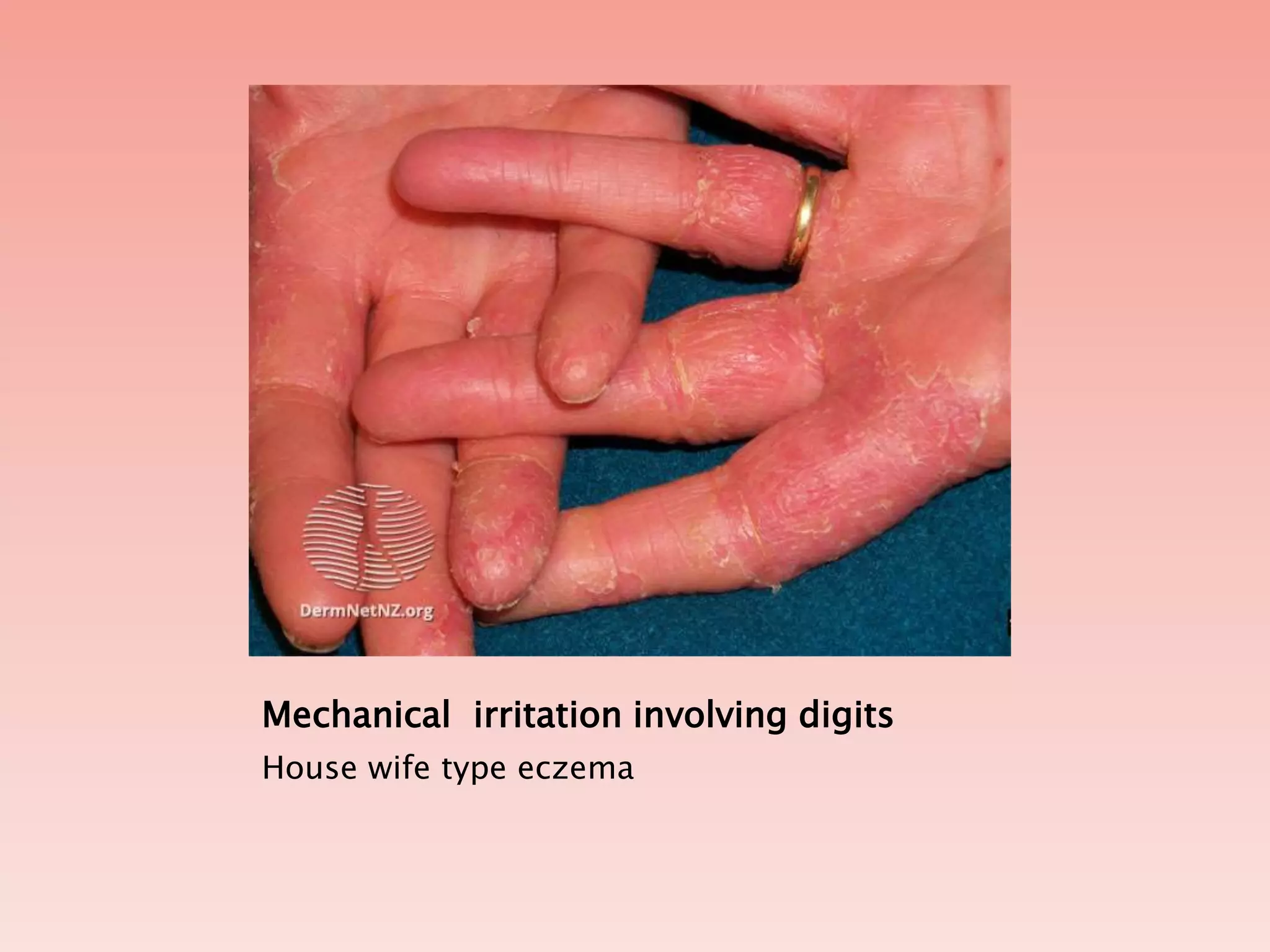










Irritant contact dermatitis is a form of skin inflammation caused by contact with substances that damage the skin barrier. It can be caused by chemicals, environmental factors like heat and friction, or physical agents like wet work. The skin loses oils and moisture, allowing irritants to penetrate and cause inflammation. Symptoms include stinging, burning, redness, swelling and blistering. Treatment focuses on avoiding irritants, using emollients and barrier creams, and topical anti-inflammatory medications.














































































