This document summarizes information about psoriasis, including its epidemiology, genetics, clinical presentations, pathogenesis, and relationship to cardiovascular disease risk factors. Some key points:
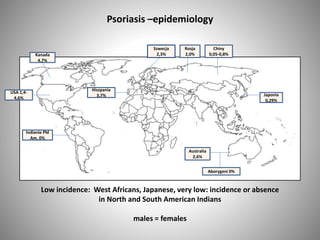
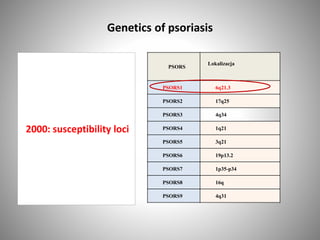
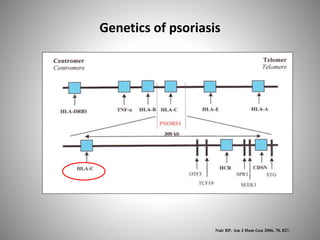
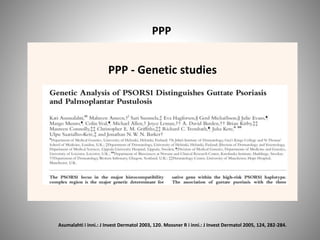
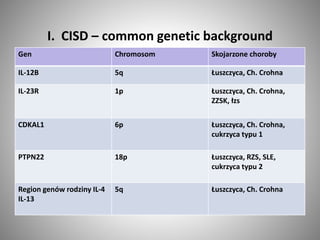
- Psoriasis prevalence varies globally, from 0.05-4.7% depending on the population. Genetic factors play a role in its development and susceptibility loci have been identified.
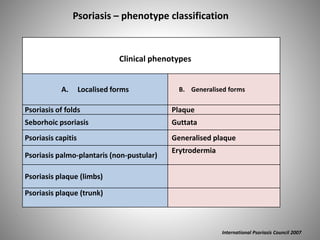
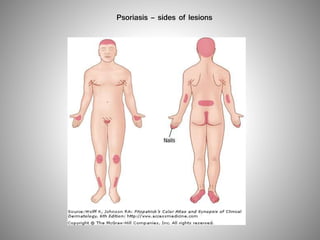
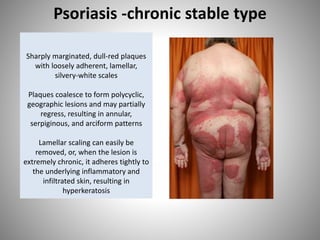
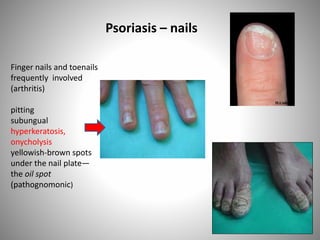
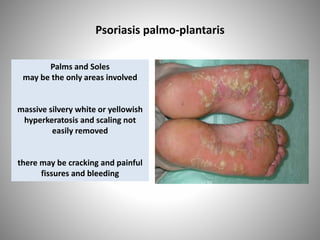
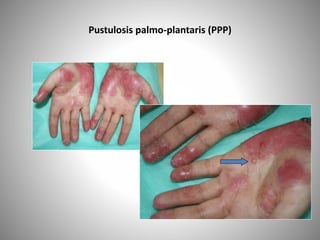
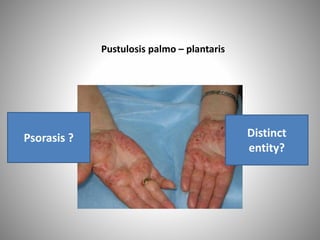
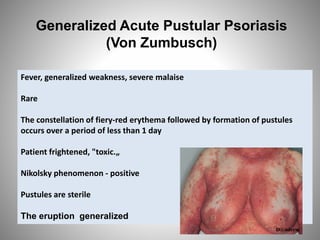
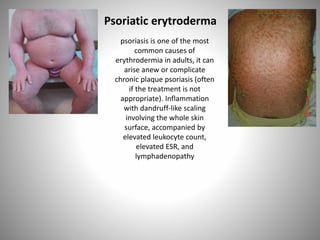
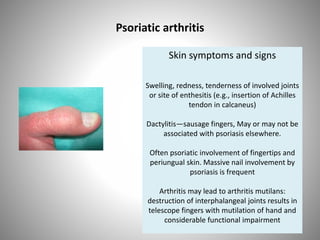
- Clinical presentations include plaque, guttate, pustular, erythrodermic, and nail psoriasis. Psoriatic arthritis affects 5-8% of patients.
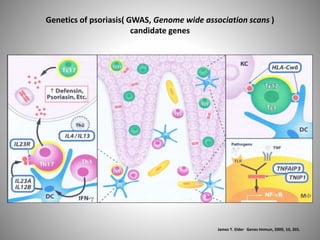
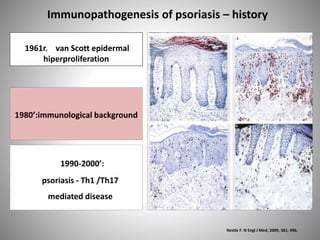
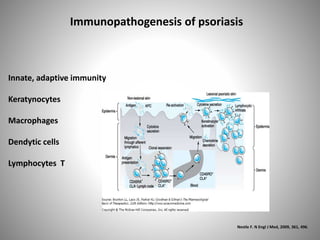
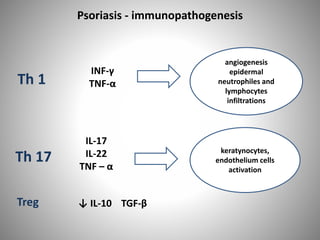
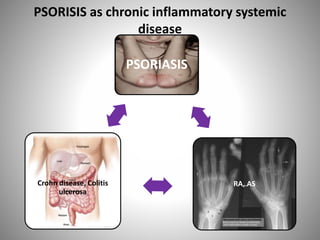
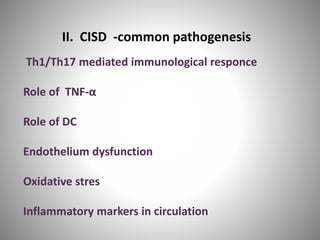
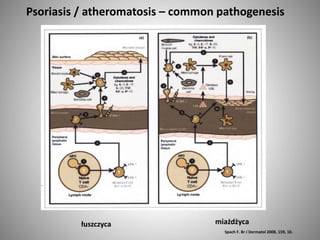
- Psoriasis is considered a T-cell mediated immune disease involving Th1 and Th17 responses and inflammatory cytokines like TNF-









![LP-etiology
Idiopathic in most cases but cell-mediated
immunity plays a major role. Majority of
lymphocytes in the infiltrate are CD8+ and
CD45Ro+ (memory) cells. Drugs, metals (gold,
mercury), or infection [hepatitis C virus (HCV)]
result in alteration in cell-mediated immunity.
There could be HLA-associated genetic
susceptibility that would explain a
predisposition in certain persons. Lichenoid
lesions of chronic graft-versus-host disease
(GVHD) of skin are indistinguishable from
those of LP](https://image.slidesharecdn.com/wbi9z2trbw1ntj2vp78o-140528233128-phpapp01/85/Psoriasis-83-320.jpg)