Downloaded 30 times




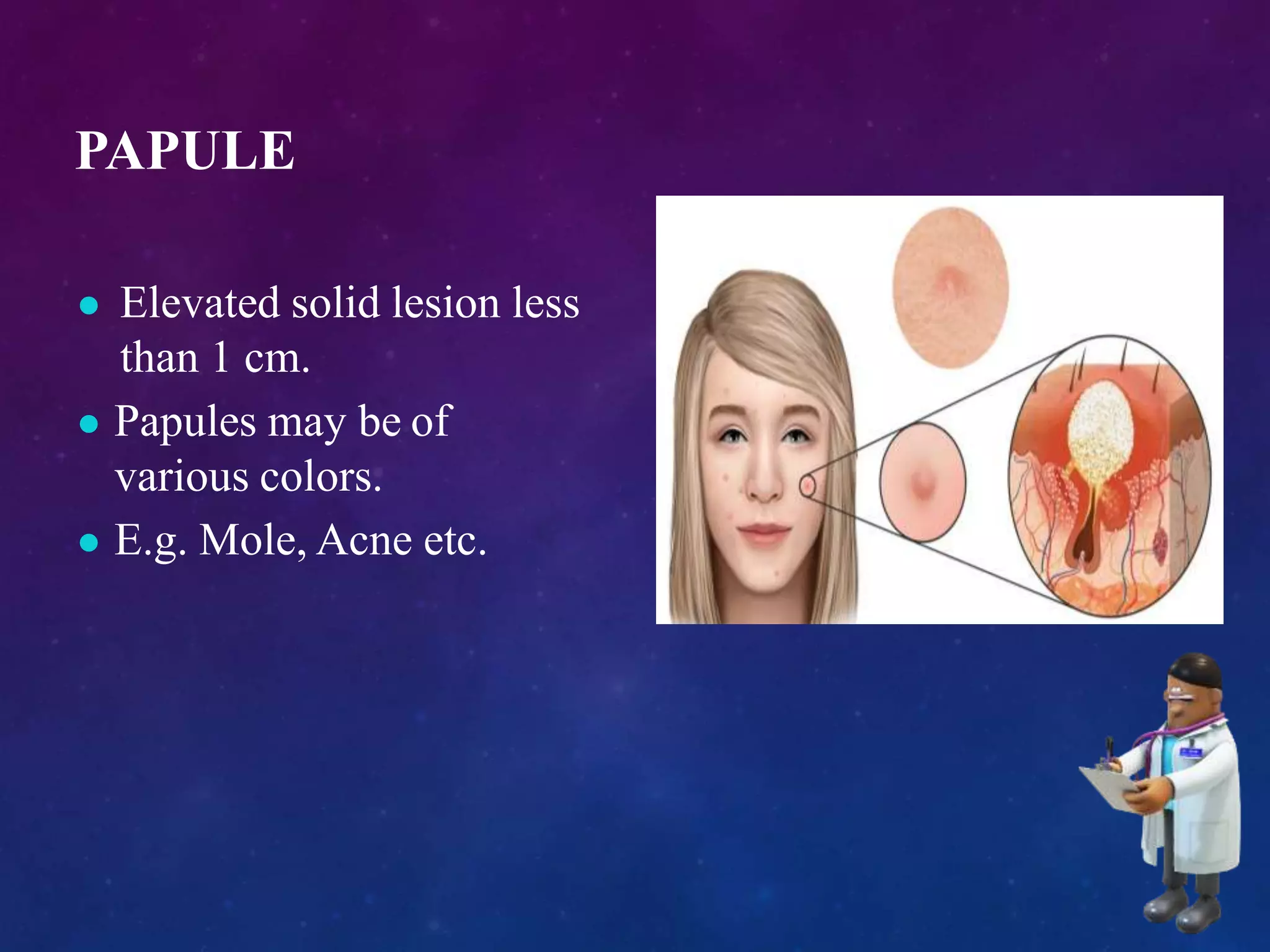





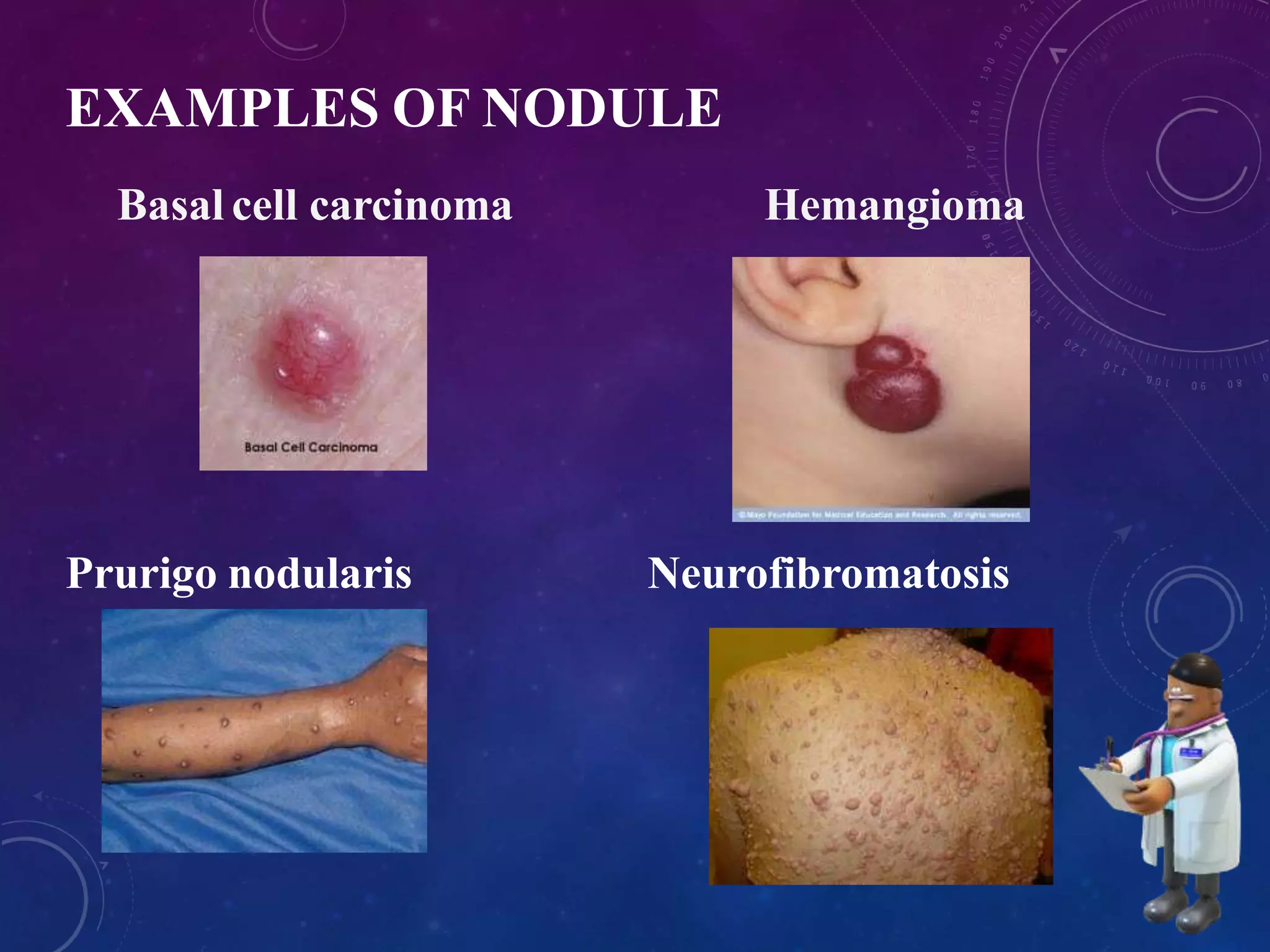

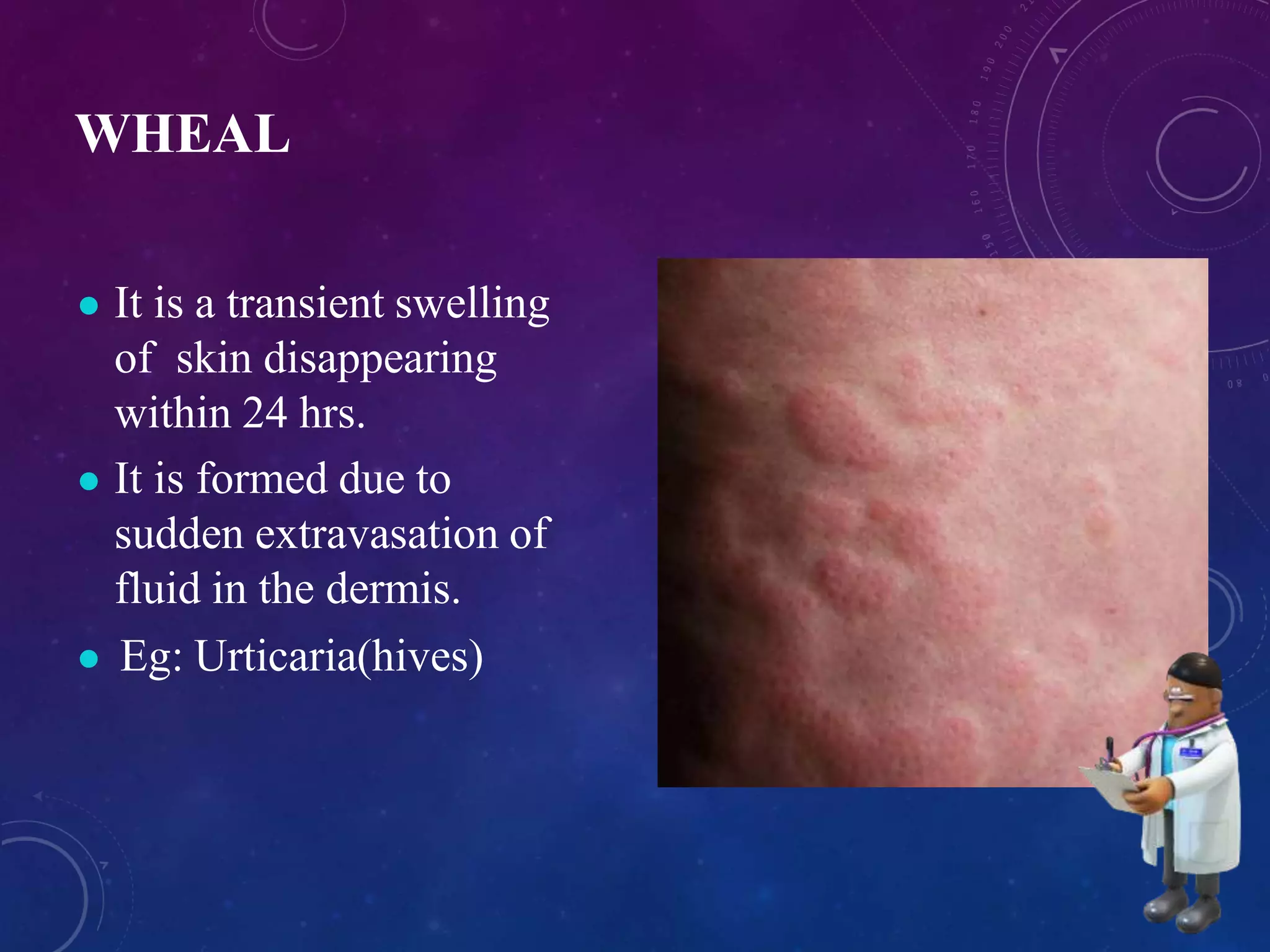
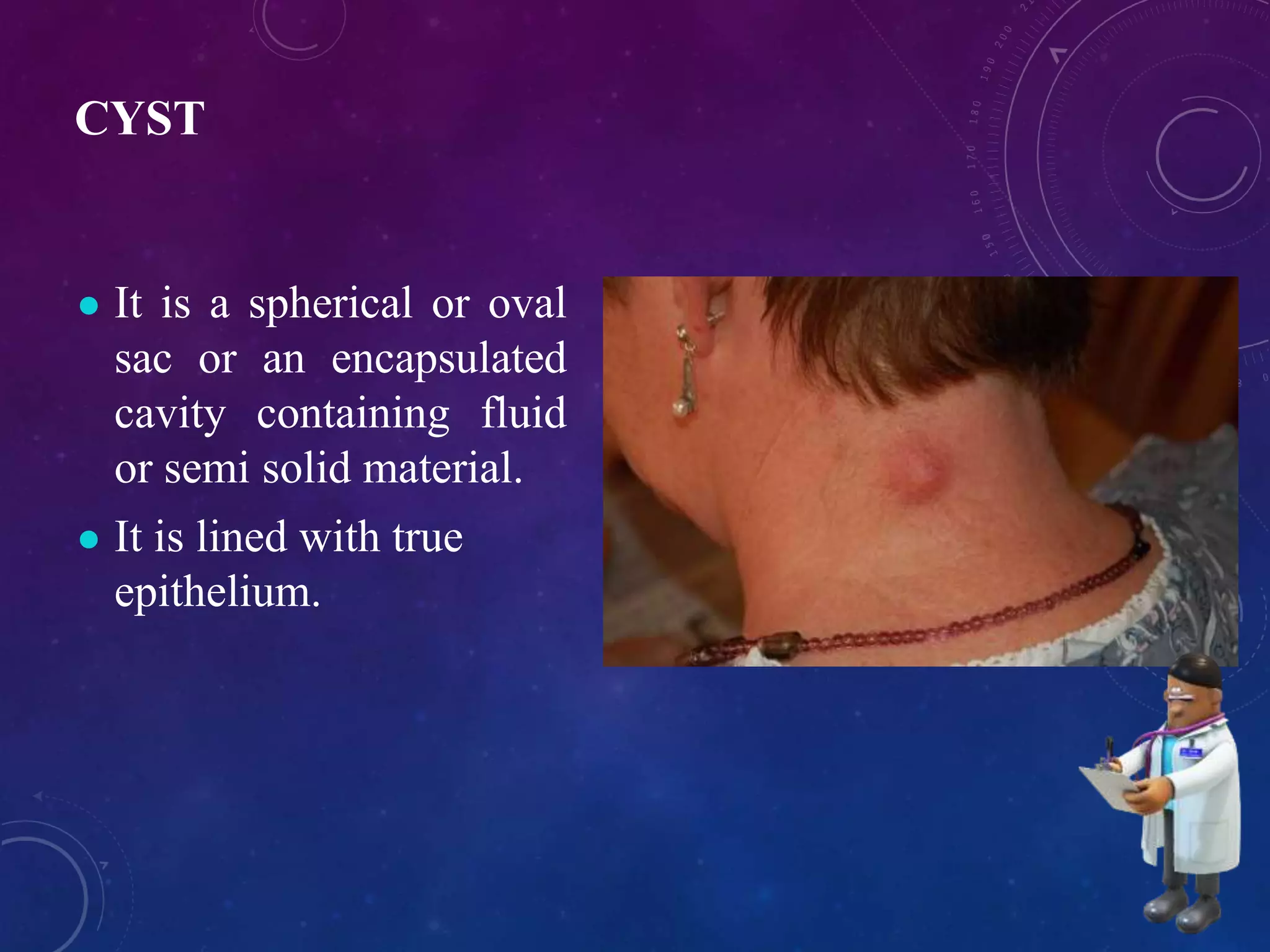

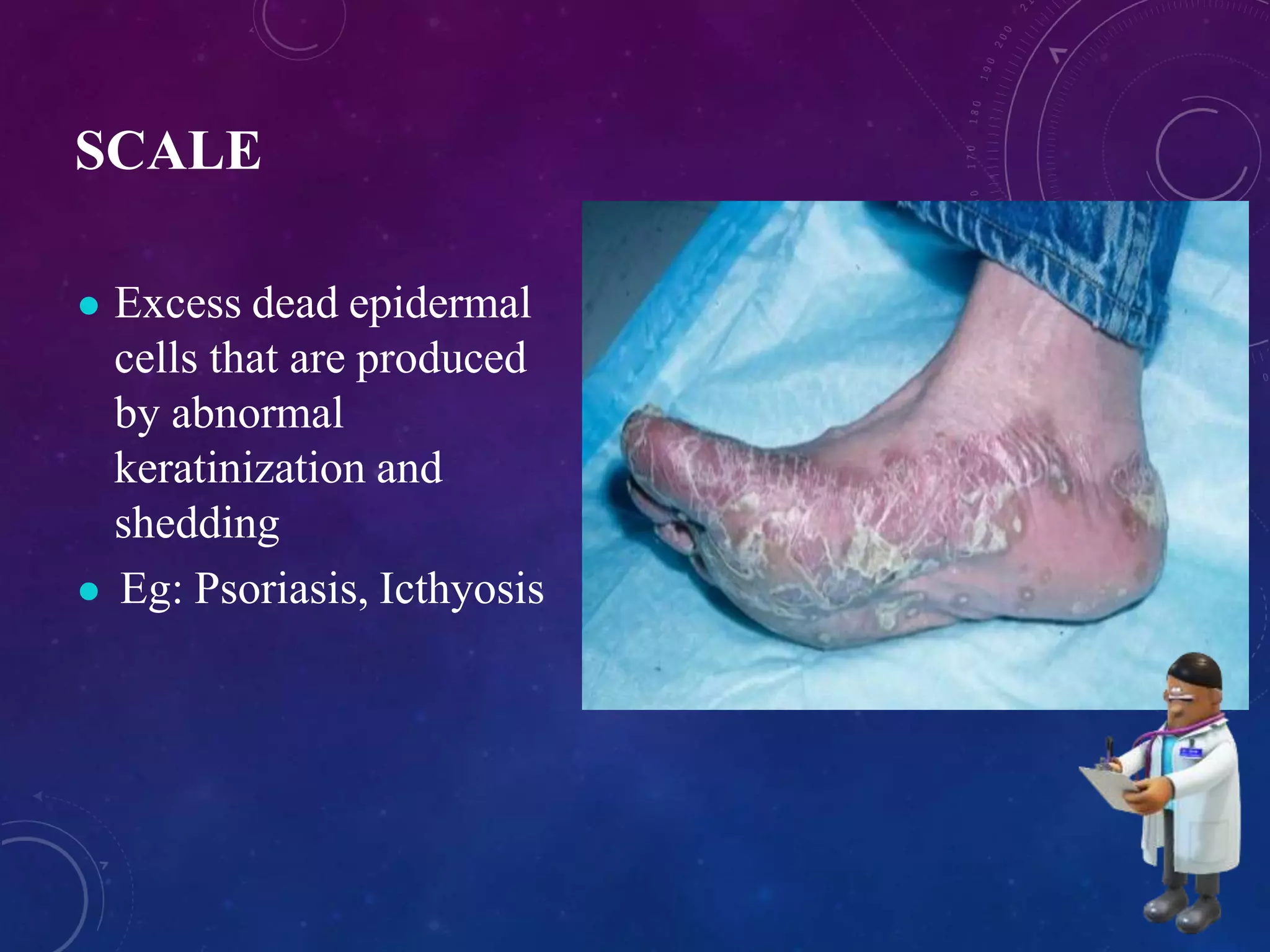

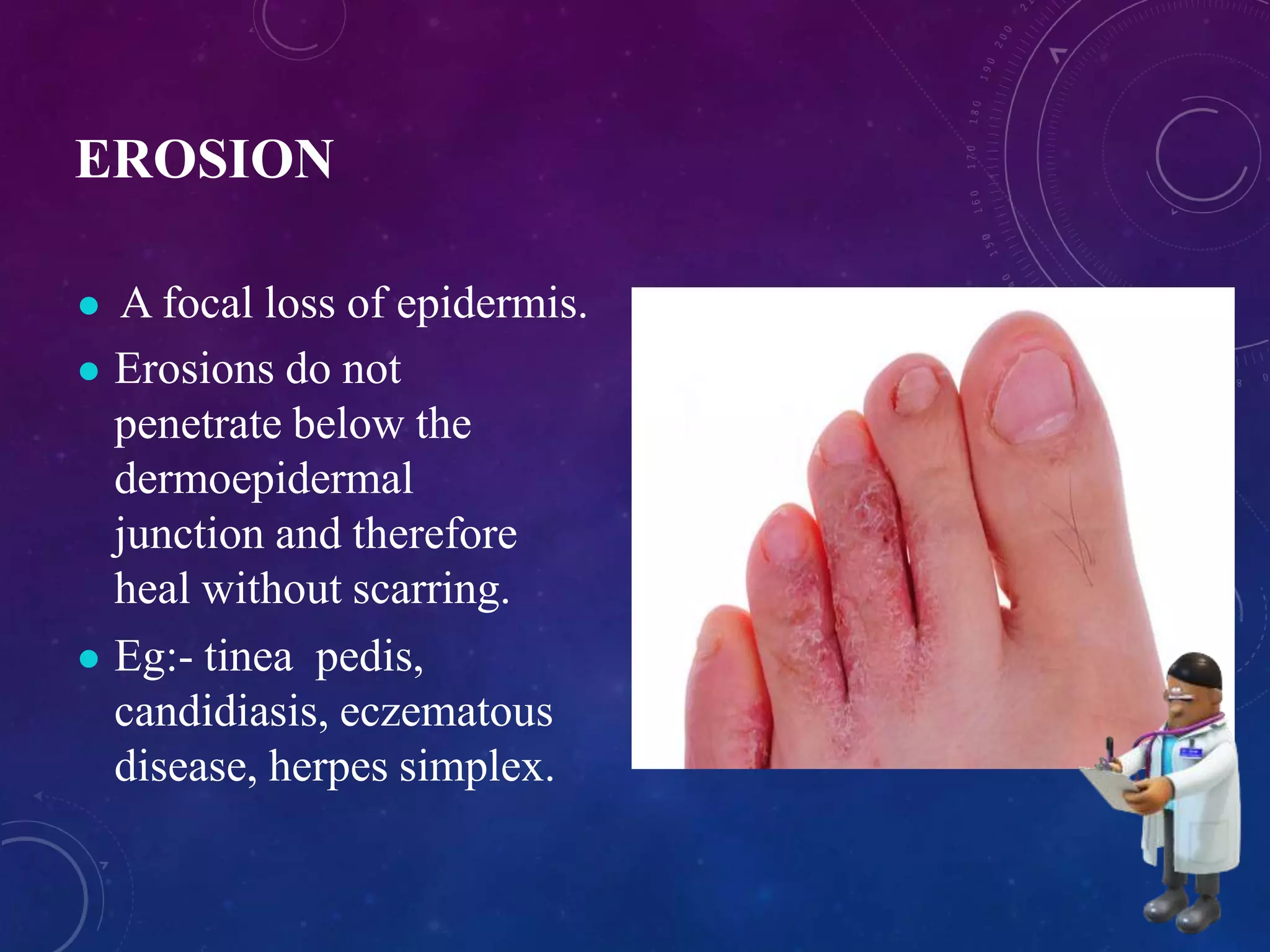
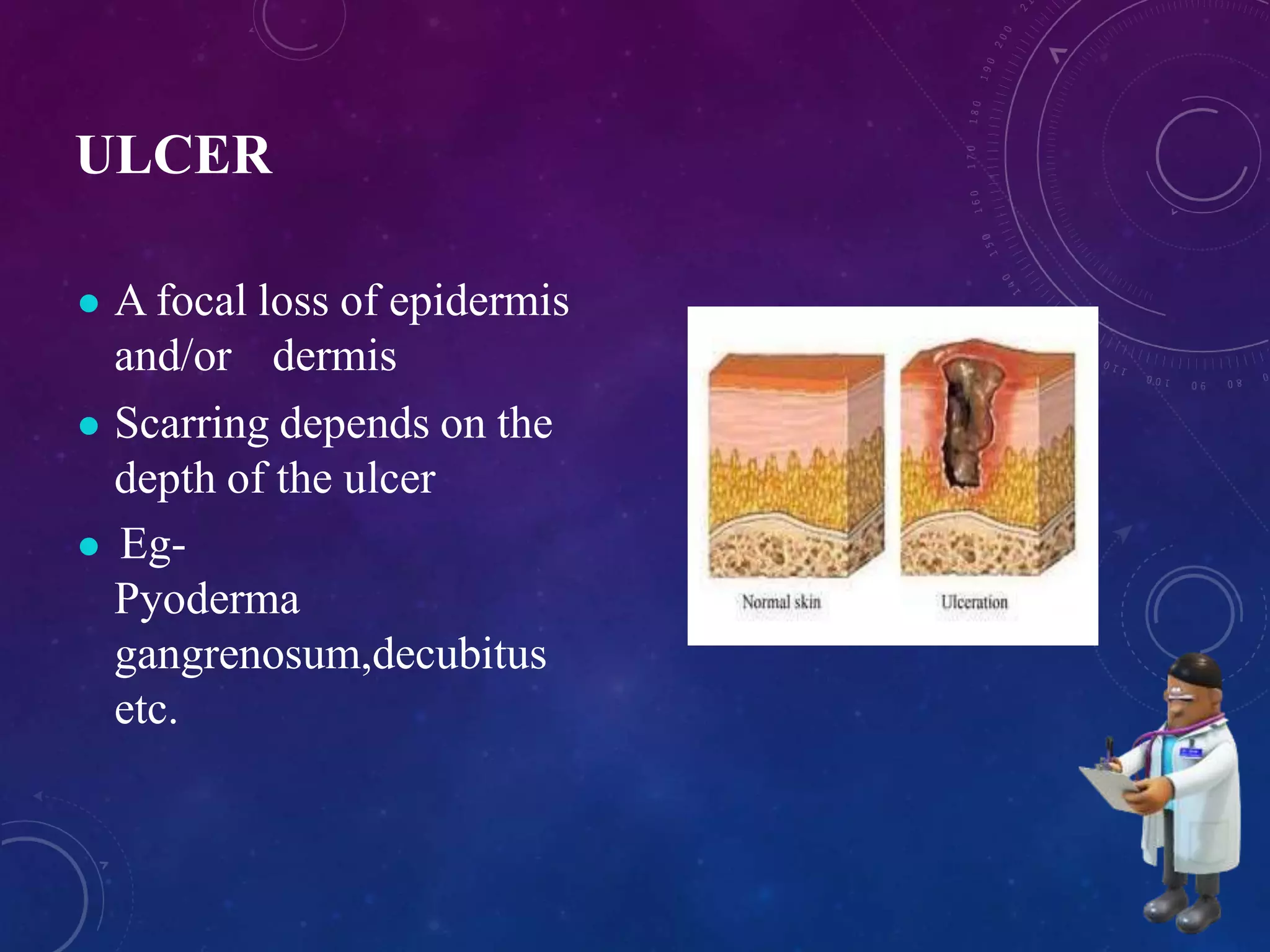




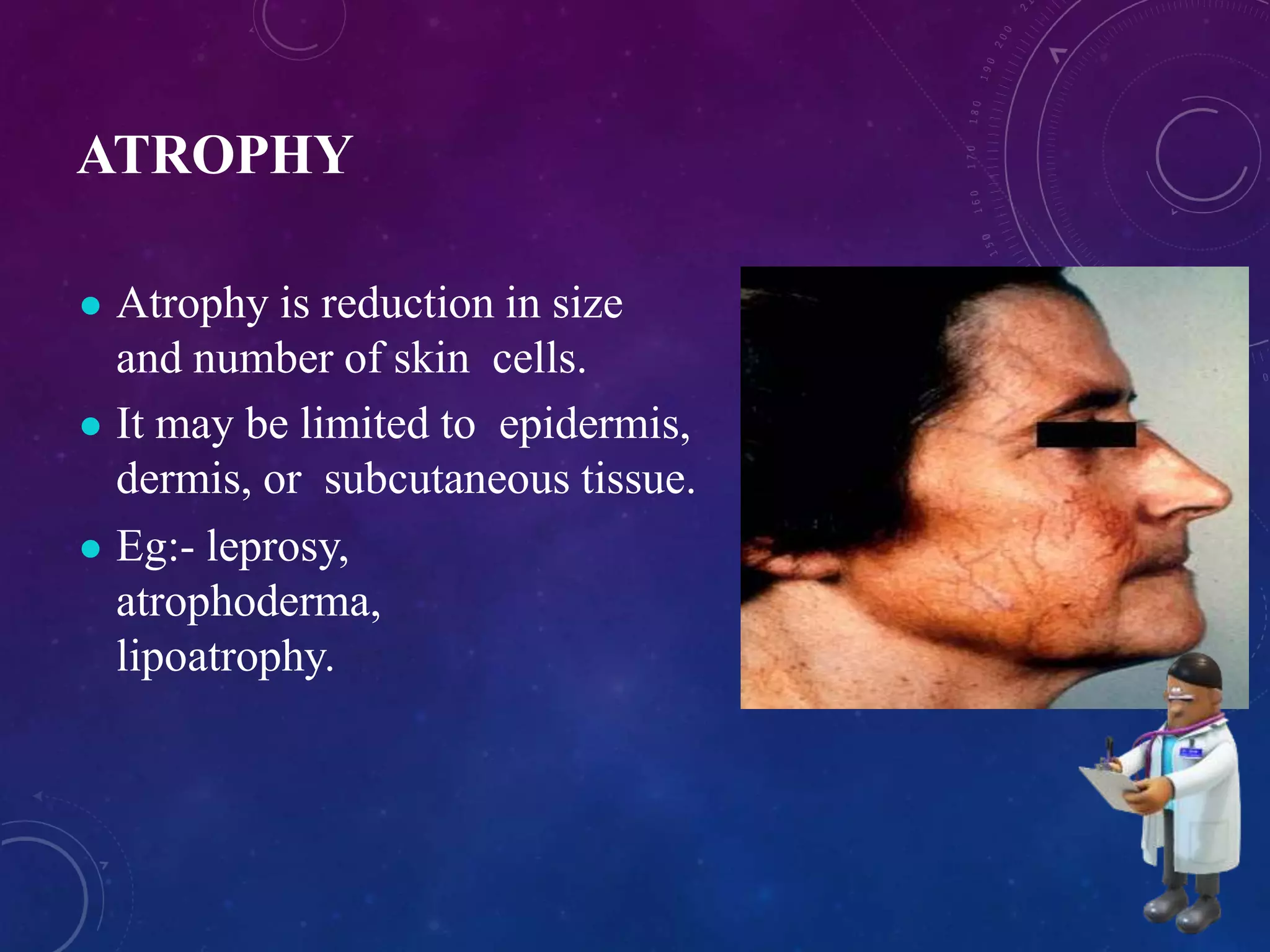






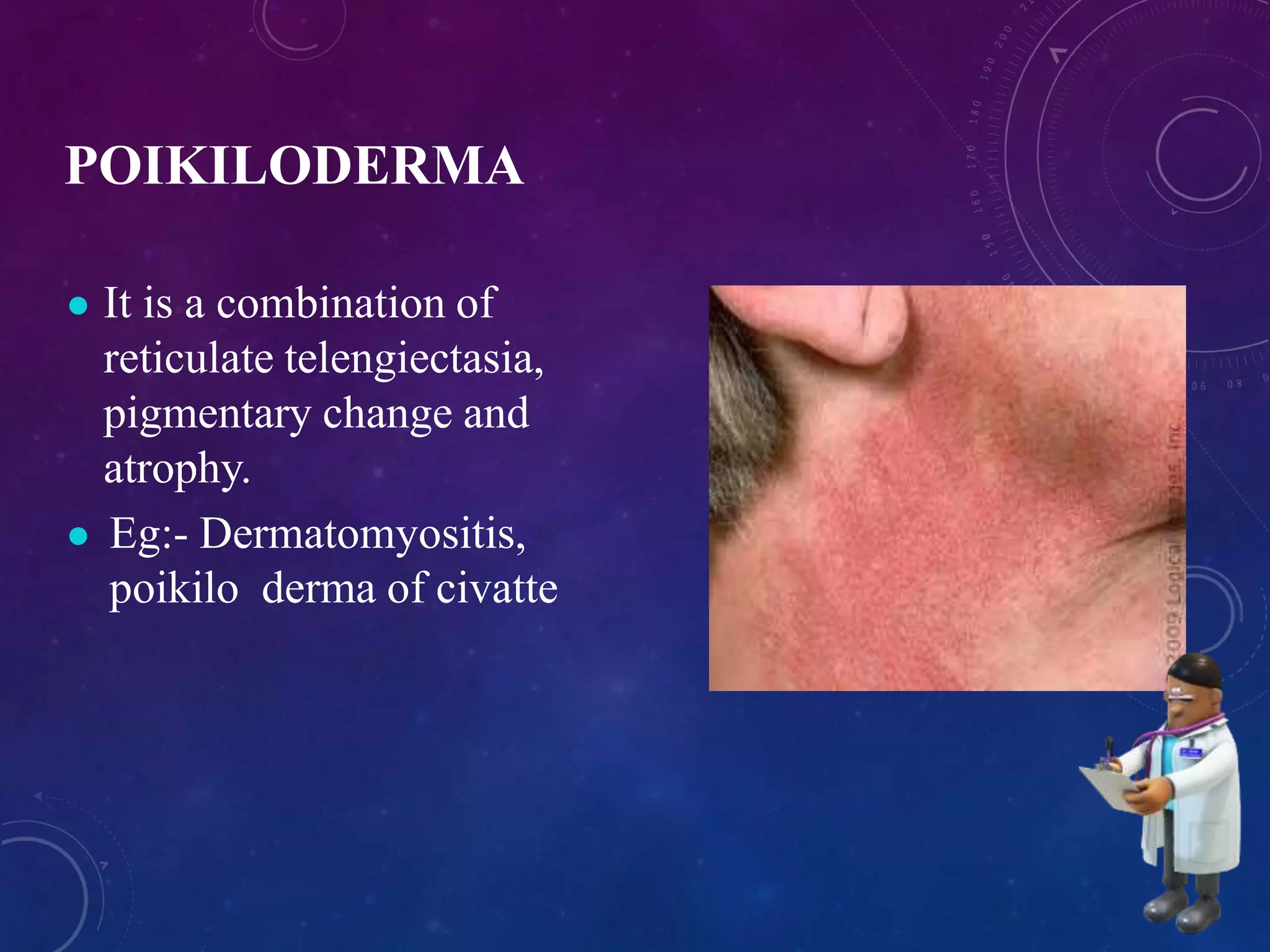



















This document describes the key features to note when describing basic skin lesions, including size, shape, color, and distribution. It categorizes lesions as primary, secondary, or special and defines common types such as macules, papules, vesicles, bullae, and pustules. Secondary lesions include scales, crusts, erosions, and fissures. The document provides examples of different lesions and explores their characteristic arrangements, colors, and predilection for specific body sites.














































































