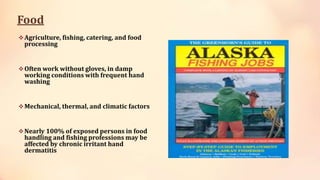
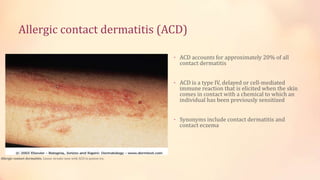
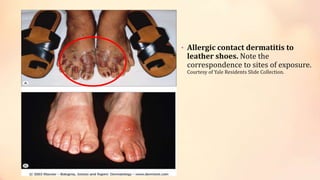
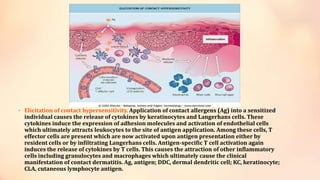
Contact dermatitis can be caused by allergic reactions (allergic contact dermatitis) or irritants (irritant contact dermatitis). Allergic contact dermatitis is a type IV delayed hypersensitivity reaction that occurs when a sensitized individual is re-exposed to an allergen. It accounts for about 20% of contact dermatitis cases. Patch testing is needed to identify the specific allergen causing allergic contact dermatitis. Irritant contact dermatitis results from direct skin damage caused by chemicals, metals, fabrics, or other irritating substances. Avoiding the irritating or allergenic substance is the primary treatment approach for both types of contact dermatitis.

![Types of Dermatitis
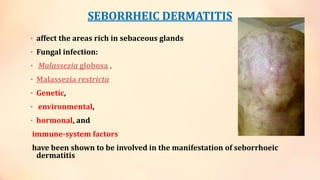
• SEBORRHEIC DERMATITIS [Skin eruptions on face, scalp, and
trunk of body. This symptoms will produce greasy, dry scales
and will appear reddish.]
• CONTACT DERMATITIS [The appearance of skin vesicles that
burn, itch , sting or scale. ]
• ATOPIC DERMATITIS [There will appear lesions on the face,
neck, knees, elbows, trunk of body.]](https://image.slidesharecdn.com/contactdermatitis-130920140849-phpapp01/85/Contact-dermatitis-4-320.jpg)