
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Psoriasis
Similar to Psoriasis (20)
More from ZeelNaik2
More from ZeelNaik2 (19)
Recently uploaded
Recently uploaded (20)
Psoriasis
- 1. PSORIASIS DR.ZEEL NAIK Assistant Professor , Maliba Pharmacy College, UTU.
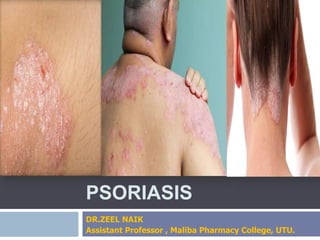
- 2. PSORIASIS Psoriasis is a common chronic inflammatory skin disorder characterized by recurrent exacerbations and remissions of thickened, erythematous, and scaling plaques.
- 3. PSORIASIS The word psoriasis is derived from Greek word ‘psora’ means ‘itching’. Psoriasis is a chronic , non- infectious , inflammatory disease of the skin in which epidermal cells are produced at a rate that is about 6-9 times faster than normal. The cells in the basal layer of the skin divide too quickly and the newly formed cells move so rapidly to the skin surface that they become evident as profuse scales or plaques of epidermal tissue.
- 4. PSORIASIS The psoriatic epidermal cells may travel from the basal cell layer of the epidermis to the stratum corneum and with in 3-4 days, which is in sharp contrast to the normal 26-28 days.
- 5. PSORIASIS It is a chronic inflammatory disorder of skin that affects approximately 2%-3% of the population. Common sites affected include the scalp, buttocks, elbows, knees, hands , legs and nails. Although it is often limited to skin, up to 25% of patients also have am associated psoriatic arthropathy and moderate to severe psoriasis is associated with the risk of CVS disease and death.
- 7. EPIDEMIOLOGY Psoriasis, a chronic proliferative skin disease is one of the most common immune mediated disorders occurring in 2- 3% of population world wide. Of patients, 75% present with symptoms of psoriasis before age 45yrs. Although rarely life-threatening, psoriasis has an adverse physical and emotional impact on quality of life. It affects both sexes equally and can occur at any age. Most commonly appears for the first time between the ages of 15 and 35 years. The study found 35% of people with psoriasis could be classified as having moderate to severe psoriasis.
- 8. Etiology Idiopathic Cause : It means disease or condition which arises spontaneously or for which the cause is unknown. Some of the factor that may trigger psoriasis are : Genetic Autoimmune Reaction Infection Injury to Skin Change in climate. Medications. Stress(Physical and emotional). Obesity Smoking and Alcohol.
- 9. Etiology Bacteria or Viral infections including strep throat and upper respiratory tract infection. Dry air and dry skin. Injury to the skin, including cuts, burns and insect bites. Too little sunlight. Too much sunlight (sunburn). AIDs Rheumatoid Arthritis Cancer Chemotherapy. Koebner Phenomenon
- 10. ETIOLOGY Psoriasis is a complex and multifactorial disease that is apparently associated with interaction between environmental factors (exogenous or endogenous antigens) and a specific genetic background. It is not contagious and cannot be spread to others. It occurs when body's immune system mistakes healthy cells for dangerous substance.
- 11. ETIOLOGY Usually, skin cells grow deep in the skin and rise to the surface about once a month. In persons with psoriasis, this process is too fast. Dead skin cells build up on the skin’s surface.
- 12. ENVIRONMENTAL FACTORS Factors such as climate, stress, alcohol, smoking, infection, trauma, and drugs can aggravate psoriasis. Alcohol seems to have a greater influence on the progression of psoriasis in men, and the association between smoking and psoriasis seems to be stronger in women. Psoriatic lesions can develop at the site of injury on normal appearing skin. This response can be induced by a variety of trauma that includes rubbing, venipuncture, bites, surgery, and mechanical pressure. Lithium carbonate, β-adrenergic blocking agents, some antimalarial agents, NSAIDS, and tetracyclines are among the most commonly reported drugs to
- 13. GENETIC FACTORS There is a significant genetic component in psoriasis, but the exact mode of inheritance is uncertain. Monozygotic twins or Identical twins have a higher concordance for psoriasis than dizygotic or fraternal twins.
- 14. Pathophysiology Etiologic Factors The skin in the patches of psoriasis is growing much faster than normal skin Rapid production of cells which does not allow the cells to manufacture a keratin that gives its hard surface. Flaking and patches of skin.
- 15. Pathophysiology (2) Stress, Genetic, Autoimmune reaction and Medication cause. Hyper activation of T-cells. Epidermis Infiltration and Keratinocyte Proliferation Deregulated Inflammatory Process
- 16. Large Production of various cytokines (Interferon γ, IL-2,IL-12,IL-17,IL-23 TNF- α, IL-8 and others) Superficial Blood vessel dilated and vascular engorgement. Epidermal hyperplasia and improper cell maturation.
- 17. PATHOPHYSIOLOGY The three key steps involved in the pathogenesis of psoriasis are i. T-cell activation by antigen in the lymph nodes ii. T-cell binding to the endothelium in the vasculature, with subsequent migration into the dermis and epidermis iii. T-cell reactivation by a second exposure to antigen, which occurs in the dermis. Certain CD4+ and CD8+ T cells have a marker on their cell surface known as cutaneous lymphocyte antigen (CLA) • These CLA-positive T cells are recruited from the circulation and migrate to the skin during inflammatory processes and have been implicated in the pathogenesis of various skin diseases, including psoriasis • For these T cells to become activated, an APC(antigen presenting cell) presents antigen to the T-cell receptor.
- 19. Clinical Presentation and Diagnosis Most patients with psoriasis have symptoms of the disease throughout their lifetime. Patients who experience frequent relapses, occurring within months or even weeks, tend to develop more severe disease. The palm of one's hand, from the wrist to the fingertips, represents approximately 1% of the body surface area (BSA). Disease affecting less than 2% of the BSA is considered mild, moderate psoriasis involves 3% to 10%, and severe psoriasis involves more than 10% of the BSA.
- 21. Classification
- 22. Classification Psoriasis Vulgaris or Plaque Psoriasis. Guttate Psoriasis. Inverse Psoriasis or Flexular Psoriasis. Pustular Psoriasis or palmoplantar Psoriasis. Erythrodermic Psoriasis. Nail Psoriasis. Psoriatic Arthritis.
- 24. Psoriasis Vulgaris or Plaque Psoriasis Psoriasis vulgaris or plaque psoriasis, the most common form of the disease, affects approximately 80% of psoriasis patients. Lesions are usually distributed in a symmetrical pattern, typically located on the scalp, the lumbar region of the back, and the extensor surfaces of the elbows and knees. The well-demarcated erythematous plaques covered with silvery scales range in diameter from less than 1 cm to 10 cm. The lesions are associated with pain and pruritus (itching) and can occasionally crack and bleed. Scale removal may result in punctate bleeding, also called the Auspitz sign.
- 25. Psoriasis Vulgaris or Plaque Psoriasis
- 26. Guttate Psoriasis Guttate psoriasis commonly affects children and young adults and is often associated with recent streptococcal infections. The lesions are usually small, scaly, and teardrop-shaped and typically are localized to the trunk, limbs, and scalp. Small , pink red spots appear on the skin.
- 27. Inverse Psoriasis Inverse psoriasis is a form of psoriasis that often exclusively involves the body folds. Lesions usually present in the axillae, groin, inframammary folds, navel, intergluteal crease, and glans penis areas. Inverse psoriasis presents as a large, smooth, dry, and very erythematous lesion. This type of psoriasis is more common in obese patients.
- 28. Pustular Psoriasis Pustular psoriasis is distinguished by the development of white pustules encircled by red skin. The pustules contain non-infectious pus and are usually localized to the palms and soles. Generalized disease affecting the entire body often requires hospitalization and can be fatal.
- 29. Erythrodermic Psoriasis Erythrodermic psoriasis is an acute inflammatory, erythematous, scaling disorder involving the entire skin surface Severe erythrodermic psoriasis and generalized pustular psoriasis are associated with the loss of the protective functions of the skin. These conditions are life-threatening because of the potential for systemic infections, loss of thermoregulation, and cardiovascular or pulmonary complications.
- 30. Psoriatic Arthritis Psoriatic arthritis is a chronic, progressive, inflammatory arthritis that affects as many as about 30% of patients with psoriasis.The arthritic symptoms are often associated with the development of skin lesions and include pain, swelling, and stiffness in the joints. Furthermore, approximately 5% to 10% of those patients may experience functional disability.
- 31. Nail Psoriasis Commonly seen along with psoriatic arthritis. It appears as a pitting , small bit nail, yellow brown nail, tender and painful nail with chalk like debris build up under nails Keep the nail short and trimmed
- 32. CLINICAL MANIFESTATION Irritated , red, flaky patches on the skin. Most often seen on elbows, knees and middle of the body. The skin is itchy, dry and covered with silver flaky skin(scales). Skin pink-red in color, raised and thick. Genital lesions in male. Joint Pain or aching. Nail Changes. Severe dandruff on the scalp. Burning sensation on the skin. Cracked and bleeding skin Pus filled blisters. Pitting, small depression on the surface of the nail.
- 33. CLINICAL MANIFESTATION Restricted joint motion or pain. Bilateral symmetry is a feature of psoriasis. In approximately 25-50% of psoriasis patient, nails are involved , with pitting , discoloration , crumbling beneath the free edges and separation of the nail palate.
- 35. Psychosocial Aspects Physical and psychological disability produced by the disease may range from minor to total. Severe psoriasis is associated with substantial morbidity and can cause functional impairment, skin disfigurement, and emotional distress. Approximately 30% of patients with psoriasis have moderate to severe disease. The prevalence of depression and suicidal ideation among patients with psoriasis is consistent with figures seen in other populations with chronic illness. Psoriasis directly affects the quality of life and may cause difficulty in work performance, problems with social rejection, sexual dysfunction, and depression.
- 36. DIAGNOSTIC INVESTIGATIONS COLLECT HISTORY(Onset and duration of lesions, family history of psoriasis, presence of exacerbating factors, exposure to chemicals and toxins and allergies of food, drug and environment). PHYSICAL EXAMINATION SKIN BIOPSY RADIOGRAPHY TEST TO RULE OUT PSORIATIC ARTHRITIS. BLOOD TEST FOR PSORIATIC ARTHRITIS (ESR, CRP)
- 37. GOALS OF MANAGEMENT TO SLOW THE RAPID TURNOVER OF EPIDERMIS. TO PROMOTE RESOLUTION OF THE PSORIATIC LESIONS. TO CONTROL THE NATURAL CYCLES OF THE DISEASE THERE IS NO KNOWN CURE OF THIS DISEASE OR DISORDER. AVOID ANY PRECIPITATING OR AGGRAVATING FACTORS. AN ASSESSMENT IS MADE OF LIFESTYLE , BECAUSE PSORIASIS IS SIGNIFICANTLY AFFECTED BY STRESS.
- 38. TREATMENT Psoriasis treatment is divided into 4 main types : 1. Topical Therapy e.g. Corticosteroids,Vitamin D analogues, Coal Tar. 2. Phototherapy e.g. UVB, PUVA 3. Systemic Therapy e.g. Methotrexate,Azathioprine, Cyclosporin, Acitretin,Hydroxyurea.
- 39. TREATMENT CHART
- 40. TREATMENT
- 41. Topical Therapy Topical therapy are first-line treatments for mild to moderate psoriasis and can often be used in combination with systemic treatments in more severe psoriasis. Different formulations such as ointment, creams and gels should be used.
- 42. 1st LINE TOPICAL PHARMACOTHERAPY 1. KERATOLYTICS Salicylic acid is most commonly used keratolytics. It causes a disruption in corneocyte to corneocyte cohesion in the abnormal horny layer of psoriatic skin. This helps to remove scales, smooth the skin, and decrease hyperkeratosis. The keratolytic effect enhances the penetration and efficacy of some other topical agents such as corticosteriods. It is applied as a 2% to 10% gel or lotion 2 – 3 times a day. Salicylic acid produces local irritation.
- 44. 2. Topical Corticosteriod They halt synthesis and mitosis of DNA in epidermal cells and appear to inhibit phospholipase A, lowering the amount of prostaglandins and leukotrienes in the skin. These causes vasoconstriction , reduce erythema, pruritus and scaling. Improvement is usually achieved within 2-4 weeks. They slow the cells turnover by suppressing the immune system which reduce inflammation and relieves from associated itching.
- 45. Topical Corticosteriods Low potency products (e.g. hydrocortisone 1%) have a weak anti inflammatory effect and are safest for long term application and are recommended for sensitive area. Medium Potency Products are used in moderate inflammatory lesions. High Potency Preparations are used primarily as alternative to systemic corticosteriods when local therapy is feasible. Very High Potency Products may be used for thick, chronic psoriatic lesions but for only short periods of time and on relatively small surface areas. Ointments are the most effective formulation for psoriasis because they have an oily phase that conveys a hydrating effect and enhances penetration of the corticosterioid. They are not suited for use in the axilla, groin or intertriginous areas where maceration and folliculitis may develop.
- 46. Topical Corticosteriod Creams are more cosmetically desirable for some patients. They may be used intertriginous areas even though their lower oil content makes them more drying than ointments. Topical corticosteroids can be applied 2-4 times a day daily.
- 47. Corticosteriod Brand Name Strength Relative Strength to hydrocortisone Hydrocortisone (0.5-2.5%) Hydrocortisone Mild 1 Fluocinolone Acetonide (0.0025%) Synalar 1:10 Mild 1 Betamethasone Valerate (0.025%) Betnovate RD Moderately Potent 2.5 times stronger Clobetasone butyrate (0.05%) Eumovate Moderately Potent 2.5 times stronger Fluocinolone Acetonide (0.00625%) Synalar 1:4 Moderately Potent 2.5 times stronger Fludroxycortide Haelan Moderately Potent 2.5 times stronger Betamethasone Valerate (0.1%) Betnovate Highly Potent 10 times stronger Mometasone Furoate (0.1%) Elocon Highly Potent 10 times stronger Clobetasol Propionate (0.05%) Dermovate Very Potent 50 times stronger
- 48. TOPICAL CORTICOSTEROIDS 50 g of ointment or cream may be used per week. Recommended amount of a topical corticosteriod corresponding to one finger tip. The finger tip unit (FTU) is equivalent to approximately 0.5 grams of cream/ointment and should cover a skin area of about 2 % body surface area.
- 50. ADRS of TOPICAL CORTICOSTEROIDS Local tissue atrophy , skin degeneration and striae. Thinning of the epidermis and purpura. The use of potent corticosteroids may cause systemic absorption and include risk of hyperglycemia and development of cushingoid features. Tachyphylaxis(Drug Tolerance) and rebound flare of psoriasis after abrupt cessation of therapy can also occur.
- 51. 3. Vitamin D Analogues Vitamin D and its analogues inhibit keratinocyte differentiation and proliferation and have anti inflammatory effects by reducing IL-8, IL-2 and other cytokines. Use of Vitamin-D itself is limited by its propensity to cause hypercalcemia. Calcipotriene (Calcipotriol) Dovonex (Brand Name) is a synthetic Vitamin D analog used for mild to moderate plaque psoriasis. Improvement is usually seen within 2 weeks of treatment and approximately 70% of patients demonstrate marked improvement after 8 weeks. Calcipotriene (0.005 %) cream, ointment or solution is applied 1-2 times a day(no more than 100 g/week)
- 52. Vitamin D Analogues Calcitriol ,tacalcitol and maxacalcitol are other vitamin D derivatives that have been studied for treatment of psoriasis. Salicylic acid inactivates calcipotriene. It is often used in combination with or in rotation with topical corticosteriods in an effort to maximize therapeutic effectiveness while minimizing steroid related skin atrophy.
- 53. 4.TOPICAL TAZAROTENE Tazarotene (Tazorac, Zarotex) is a synthetic retinoid that is hydrolyzed to its active metabolite, tazarotenic acid, which modulates keratinocyte proliferation and differentiation. It is available as a 0.05% or 0.1% gel and cream and is applied once daily(usually in the evening) for mild to moderate plaque psoriasis. ADRS: Local irritation, pruritus, burning, stinging and erythema. Tazarotene is often used with topical corticosteroids to decrease local ADRs and increase efficacy.
- 55. 2nd Line Topical Treatment 1. Coal Tar Coal tar is one of the oldest(since 2000 years) topical treatments for psoriasis and has anti-inflammatory , antibacterial , antipruritic and antimitotic effects. A variety of preparations are available including bath preparations, shampoos, creams and ointment. Coal tar preparations of 2%-5% tar are available. It is directly applied to the lesions in the evening and allowed to remain in skin contact through night, It may also be used in bath water. Coal Tar can be used in combination with other products such as topical corticosteroids or UVB phototherapy. The risk of carcinogenicity is low, but there may be a high rate of non-myeloma skin cancers in patients chronically exposed to coal tar and UV light.
- 57. 2. Anthralin (Dithranol) Anthralin possesses antiproliferative activity on keratinocytes, inhibiting DNA synthesis. Anthralin is a man-made version of a natural substance found in goa powder, which is from the araroba tree. It works by slowing down the growth of skin cells. It also have anti-inflammatory effect. Therapy usually starts with low concentrations (0.1%-0.25%) with gradual increases to higher concentrations (0.5%-1%). Creams and ointment formulations are applied in the evening and allowed to remain overnight. It is an effective treatment for psoriasis and with coal tars, is one of the oldest treatments used. Anthralin can irritate normal skin and stain clothing. Short contact Anthralin therapy (SCAT) with application for 10 to 20 minutes of higher concentrations( 1%-5%) in water soluble vehicle is effective.
- 59. 2. PHOTOTHERAPY AND PHOTOCHEMOTHERAPY 1. UVB Many patients with psoriasis will report an improvement in their skin after sunny holidays, with only 10% of patient reporting deterioration in symptoms on sun exposure. Phototherapy with either UVB or photochemotherapy with UVA after psoralen exposure (PUVA) has an immunosuprresive effects on the skin and has been used to treat psoriasis. UVB light (290-320 nm) therapy is an important therapy for psoriasis. The most effective wave length is 310-315 nm which is also known as narrow-band UVB and most commonly used for moderate-severe psoriasis. It is preferable to older UVB (290-320 nm) lamps, due to increased safety and reduced risk of burning. Heat and humidity from sunlight provide additional positive effects.
- 60. 2. PHOTOTHERAPY AND PHOTOCHEMOTHERAPY Narrow-band UVB is an effective treatment for getting rapid control of widespread disease, with 75% of patients being clear or nearly clear of psoriasis after a course of treatment. Usually 2-3 treatments a week for 6 weeks. Topical and sometimes systemic psoriatic therapies are used adjunctively to hasten and improve the response to UVB phototherapy. Emollients enhance efficacy of UVB and can be applied just before treatments. Combining short contact anthralin, Calcipotriene or Tazarotene to UVB may also improve results. However, topical application should be done after or atleast 2 hours before UVB therapy because phototherapy can inactivate the topical product. Risks: sunburn, photo aging, and skin cancer.
- 61. 2. PUVA (Photo chemotherapy) It is photo chemotherapeutic approach for selected psoriasis and mainly has a role in the treatment of moderate to severe psoriasis. Psoralens (photo sensitizer) are drugs that are activated by long wave UV light(320-400 nm) which interact with DNA synthesis and reducing epidermal turnover. Photo chemotherapy combines psoralens with UVA light in the 320 to 400 nm spectrum. 2 Psoralens are available : methoxsalen or 8-MOP(8- methoxypsoralen) and 5-MOP. Psoralens are a group of photoactive compounds that on absorption of UV light, are both antiproliferative and immunomodulatory.
- 62. 2. PUVA (Photo chemotherapy) Photo chemotherapy is used to control severe, recalcitrant, disabling plaque psoriasis. After 10 to 25 treatments over 4 to 8 weeks(2- 3times a week), >80% of patients experience clearing of symptoms, which can be maintained with periodic (twice monthly) treatments. 8-Methoxypsoralen (8-MOP) is the most widely used agent, taken at an oral dosage of 0.6 to 0.8 mg/kg of body weight , 1.25 to 1.5 hours before exposure to UVA light. ADR: Erythema, blistering, nausea, lethargy, headache, pruritus, Skin Cancer(non-melanoma).
- 64. PHARMACOLOGIC THERAPY Topical treatments: Corticosteroids: beclomethasone, dexamethasone vitamin D analogues: calciprotriene Topical Retinoids: Tazarotene Coal tar Anthralin keratolytics Systemic treatments: Immunosuppressive agents: methotrexate, cyclosporin Immunomodulatory agents: Inhibitors of T-cell activation: alefacept, efalizumab TNF-alpha inhibitors: infliximab, etanercept, adalimumab Acitretin
- 65. Topical Therapy
- 66. 3.BIOLOGIC THERAPY Immunomodulatory agents: Inhibitors of T-cell activation: Alefacept, Efalizumab TNF-alpha inhibitors: Infliximab, Etanercept, Adalimumab IL-12/IL- 23 antagonist : Ustekinumab IL-17 Antagonist : Secukinumab 1. Infliximab (Remicade) 2. Etanercept (Enbrel) 3. Adalimumab (Humira) 4. Alefacept (Amevive) 5. Efalizumab (Raptiva)
- 67. 1.INFLIXIMAB (Remicade) It is a chimeric monoclonal antibody directed against TNF- alpha. Its used in the treatment of psoriatic arthritis and chronic plaque psoriasis. An advantage over other sytemic psoriasis treatments is that infliximab doesnot adversely affect the blood counts, hepatic enzyme levels or kidney function. Dose: 5 mg/kg as an IV infusion at weeks 0,2 and 6, then every 8 weeks thereafter. For psoriatic arthritis it may be used with methotrexate. ADRs: Headache, fever,chills, fatigue, diarrhea, pharyngitis, URTI , urticaria, dyspnea and hypotension.
- 69. 2. Etanercept (Enbrel) It is a fusion protein that binds TNF-alpha, competitively interfering with its interaction with cell bound receptors. Etanercept is fully humanized, thereby minimizing risk of immunogenecity. It is indicated for patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or photo therapy. Dose : The dose for psoriatic arthritis is 50 mg SC twice weekly (3-4 days apart) for 3 months followed by maintenance dose of 50 mg per week. ADRs: Local reaction at site of injection(25% pateint), Respiratory tract infection, GI infection, abdominal pain,nausea and vomiting , headaches and rash. Serious infections including TB and malignancies can occur
- 71. 3. Adalimumab (HUMIRA) It is a human immunoglobin G1 monoclonal TNF- alpha antibody. The binding of Adalimumab results in inactivation of the proinflammatory cytokine TNF-a. It is indicated for psoriatic arthritis and treatment of moderate to severe plaque psoriasis. Dose: The dose for psoriatic arthritis is 40 mg SC every other week. The dose for plaque psoriasis is 80 mg, followed by 40 mg every other week. ADRs: Infections(URTI, sinusitis), injection site reactions, head ache and rash.
- 73. 4. ALEFACEPT(AMEVIVE) It is a dimeric fusion protein that binds to CD2 on T-cells to inhibit cutaneous T-cell activation and proliferation. It is used for treatment of moderate to severe plaque psoriasis and also effective for treatment of psoriatic arthritis. Dose: 15 mg IM once weekly for 12 weeks. ADRs : Pharyngitis,chills, dizziness,nausea, headache, injection site pain and inflammation.
- 75. 5. Efalizumab(Raptiva) It is a humanized monoclonal antibody that inhibits CD11-a integrin, which is involved in T-cell activation, migration into skin and cytotoxic effect. Used for moderate to severe plaque psoriasis. DOSE: 1 mg/kg(200 mg maximum single dose) ADRs: Head ache, nausea, chills, pain, fever and asthenia. Cases of exacerbation of psoriasis on discontinuation have been reported, leading to the suggestion that continous treatment may be required to maintain disease suppression.
- 76. 6. Ustekinumab(IL-12/IL-23 antagonist) Ustekinumab is a fully human monoclonal antibody used in the treatment of moderate to severe psoriasis. It acts by binding to and blocking the cytokines IL-12 and IL-23. Dose : It is administered as a SC injection at a dose of 45 mg at baseline, week 4 and week 12. ADR: Head ache, confusion, seizures, sudden vision changes, mental/mood disorders. Brand Name: Stelara
- 77. Secukinumab (IL-17 Antagonist) It is a fully human anti IL-17 antagonist monoclonal antibody. Dose: It is administered as a SC injection at a weekly dose of 300 mg monthly maintenance dose. ADRs: Sore throat, diarrhea, URTI, Sinusisitis,oral herpes, urticaria. Brand Name: Cosentyx
- 78. 4. Systemic Pharmacotherapy Immunosuppressive agents Methotrexate Cyclosporin Tacrolimus Mycophenolate Mofetil (CellCept) 6- Thioguanine Hydroxyurea/Hydroxycarbamide Acitretin [Soriatane] (It is not immunosuppressant agent, it is a vitamin A derivative)
- 79. Systemic therapy
- 81. 1.METHOTREXATE(GOLD STANDARD) It is an antimetabolite and is indicated for moderate to severe psoriasis and psoriatic arthritis. It inhibits purine and pyrimidine synthesis, which is required for DNA synthesis. Methotrexate works by suppressing the overactive immune system that causes psoriasis. It can be administered orally, SC or IM. DOSE : The starting dose is 7.5 to 15 mg per week,increased incrementally by 2.5 mg every 2-4 weeks until response.(maximum 25 mg per week). 50% improvement is seen after 4 months of starting of treatment. ADRs: Myelosuppression, Severe nausea and vomiting, mucosal ulceration, stomatitis,malaise,headache, macrocytic anemia, thrombocytopenia, leucopenia , hepatic and pulmonary toxicity. Contraindication: Active infections, liver disease and pregnancy (teratogenic). Contraindicated in both males and females.
- 82. 2. Cyclosporine It inhibits the first phase of T-cell activation and also inhibits the release of inflammatory mediators from mast cells, basophils and polymorphonuclear cells. It is used in both severe form of psoriasis and arthritis. DOSE : The usual dose is between 2.5-5.0 mg/kg/day given in 2 divided doses. 50 % improvement is seen after 16 weeks. ADRs: Nephrotoxicity, hypertension, hypomagnesemia, hyperkalemia, alteration in LFTs, elevation in serum lipids. GI intolerance, parasthesia and gingival hyperplasia. Cummulative treatment for 2 years may increase the risk of kidney failure, skin cancer and lymphomas. Contraindications : A compromised immune system;Abnormal kidney function;High blood pressure;Cancer, or a history of cancer.
- 83. 3. ACITRETIN (RETINOID) It is a Vitamin A derivative that inhibits epidermal proliferation and effective oral agent for psoriasis, an alternative to immunosuppressive agents. It is used in severe plaque, Erythrodermic and Pustular types of psoriasis. It shows good result when combined with PUVA and UVB and topical calcipotriol. DOSE: The initial dose is 25-50 mg daily for 2-4 weeks. ADRs : Hypervitaminosis A, hepatotoxicity, skeletal changes, hair loss, lethargy, Hyperlipidemia. Contraindication: Diabetes, high cholesterol, high amount of triglyceride in the blood, mental problems, alcoholism, depression. Brand Name: Soriatane
- 84. 4. TACROLIMUS It is an immunosuppressant that inhibits T-cell activation and useful in severe chronic psoriasis. It is not approved by FDA. DOSE : Oral doses of 0.05 mg/kg daily, with increase upto 0.15 mg/kg daily. ADRs: Diarrhea, nausea, paresthesias(pins and needles), hypertension, tremor and insomnia.
- 85. 5. Mycophenolate Mofetil (CELLCEPT) It inhibits DNA and RNA synthesis and have a specific lymphocyte antiproliferative effect. Not approved by FDA. DOSE: 500 mg orally 4 times a day, up to maximum 4 g/day. ADRs: GI toxicity, Myelosuppression, flushing, Proteinuria , lymphoma and renal failure.
- 86. 6. Sulphasalazine It is an anti-inflammatory agent that inhibits 5- lipoxygenase. Indicated for psoriatic arthritis. When used alone it is not as effective as methotrexate , PUVA or acitretin. But it is highly safe. DOSE: Oral dose: 3-4 g/day for 8 weeks. ADRs : Gastric distress, nausea, vomiting and anorexia.
- 87. 7. 6-THIOGUANINE It is a purine analog that has been used as an alternative treatment for psoriasis when all therapies have failed. Dose: 80 mg twice weekly , increased by 20 mg every 2-4 weeks. The maximum dose is 160 mg three times a week. ADRs: Bone marrow suppression, GI complications and elevation in LFTs. It is less hepatotoxic compared to methotrexate so can be used in hepatically compromised patients with severe psoriasis.
- 88. 8. Hydroxyurea/Hydroxycarbamide It inhibits cell synthesis in the S phase of the DNA cycle. It is a cytotoxic immunosuppressant drug. It has similar mode of action to methotrexate. However it is less effective than methotrexate. DOSE: 1g/day, with gradual increase to 2g/day as needed. ADRs: Bone marrow toxicity , leg ulcers, megaloblastic anemia, teratogenic, liver toxicity.
- 89. NONPHARMACOLOGIC THERAPY Emollients Emollients are frequently used during therapy- free periods to minimize skin dryness that can lead to early recurrence. As lotions, creams, or ointments, emollients often need to be applied several times per day (about four times per day) to achieve a beneficial response. Adverse effects of emollients include folliculitis and allergic or irritant contact dermatitis.
- 90. NONPHARMACOLOGIC THERAPY Balneotherapy Balneotherapy is a therapeutic approach that consists of bathing in waters containing certain salts, often combined with natural exposure to the sun. Fangotherapy( MEDICINAL CLAY OR MUD BATH). CLIMATOTHERAPY: It refers to temporary or permanent reloaction of psoriasis patient to a region with a climate more favorable to recovery. Warm and moist climate is ideal for
Editor's Notes
- Profuse means abundant, ample or excessive.
- An intriginous areas is where 2 skin areas may touch or rub together.