Download to read offline

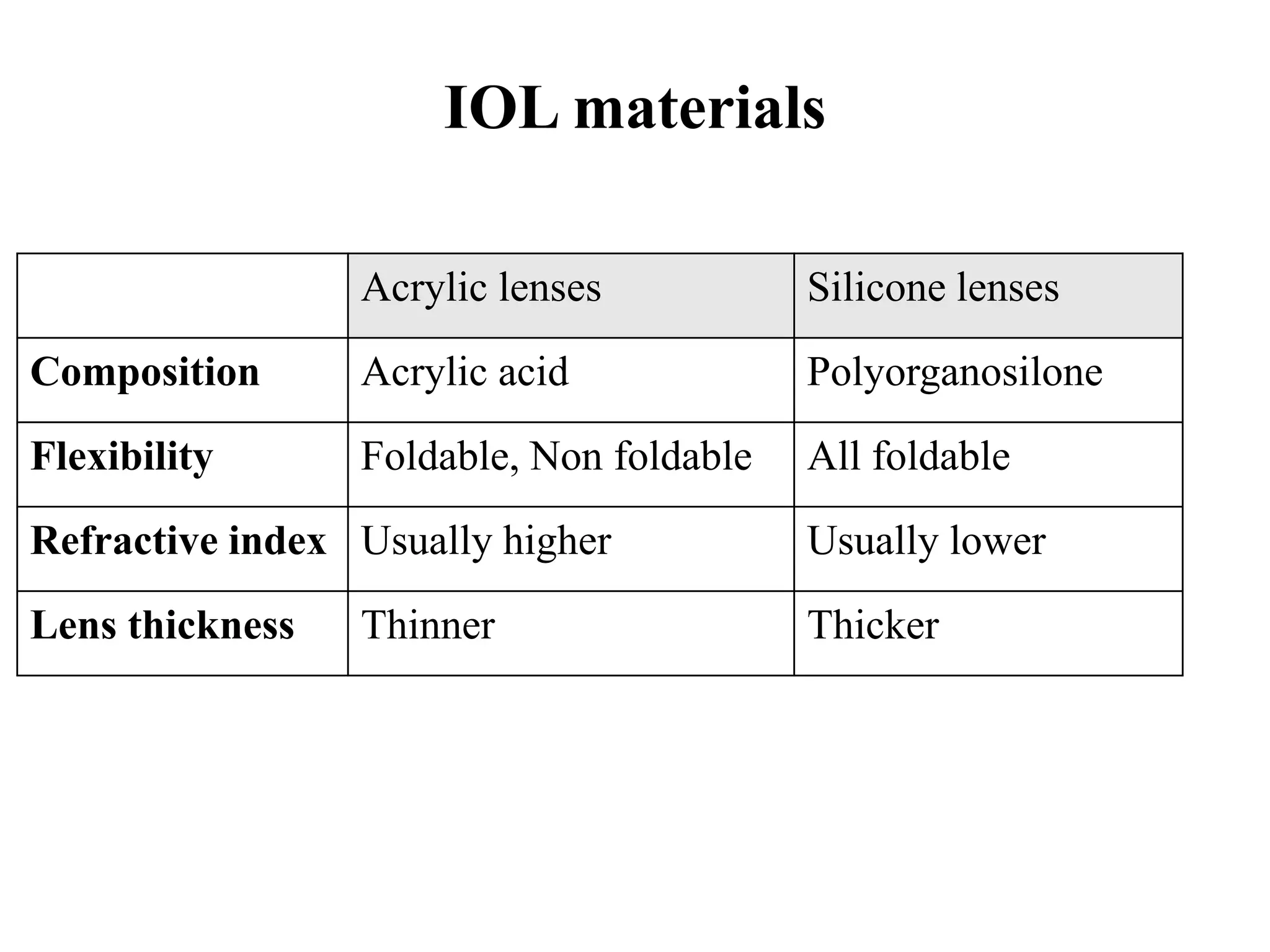
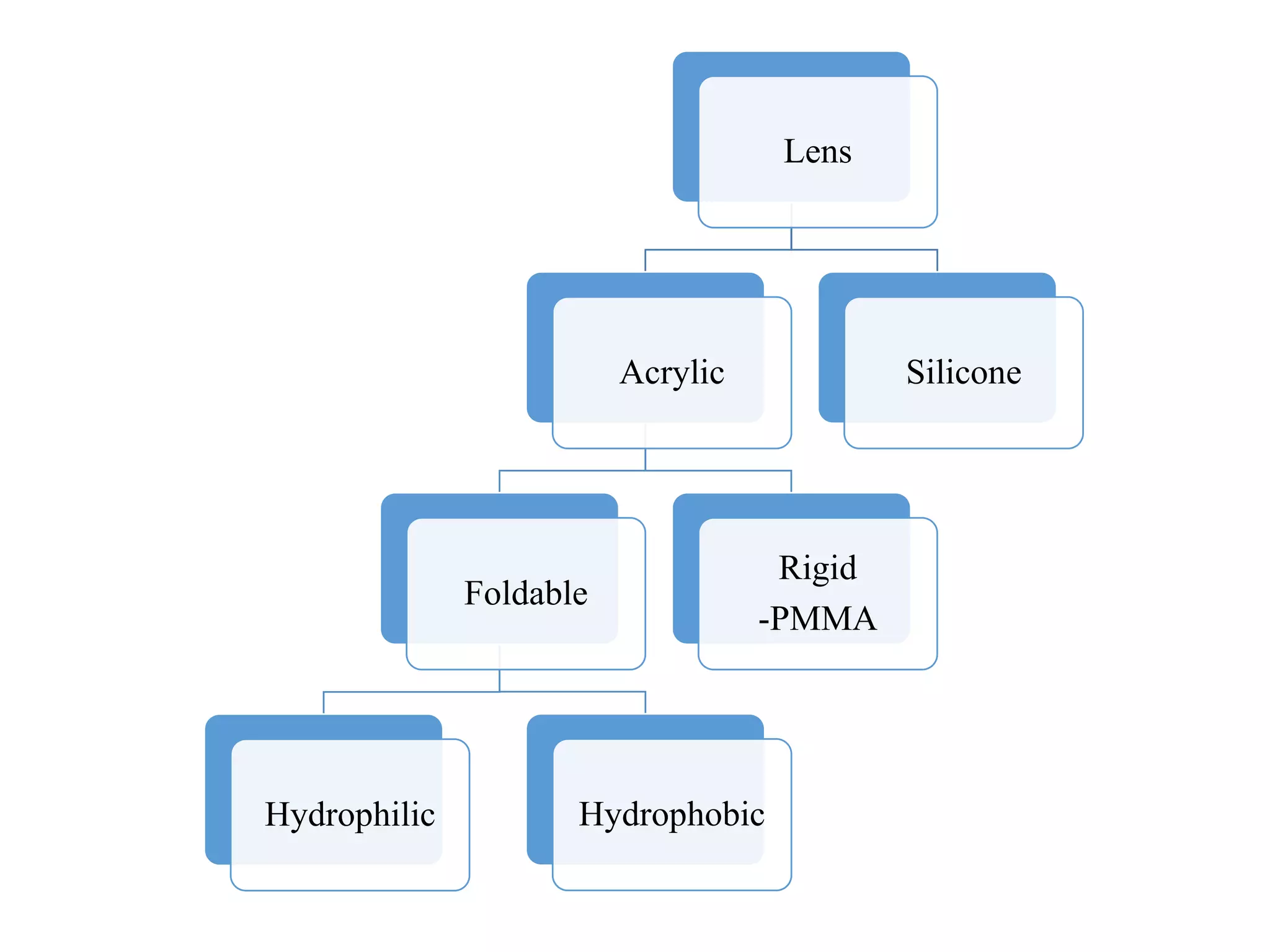
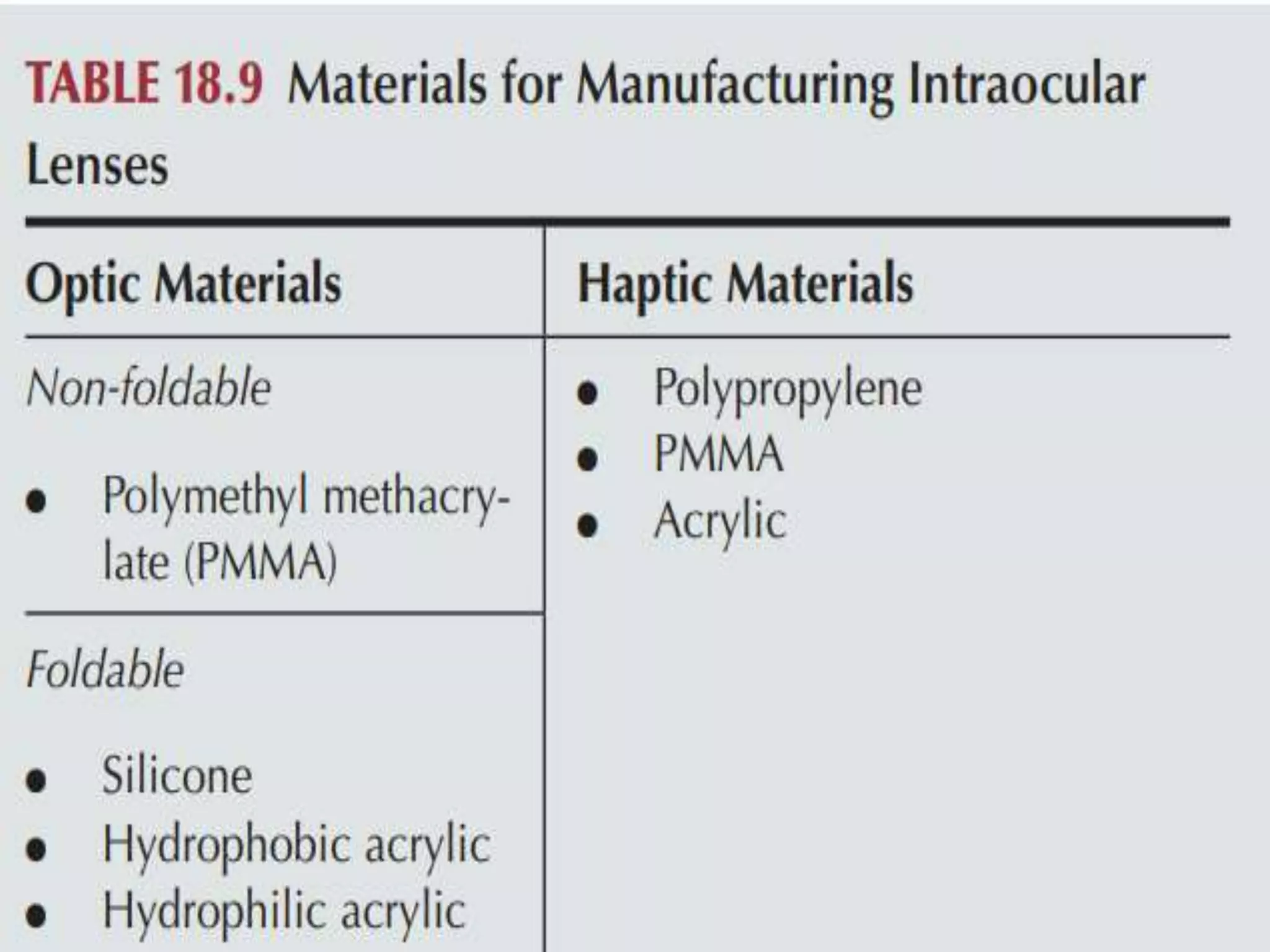
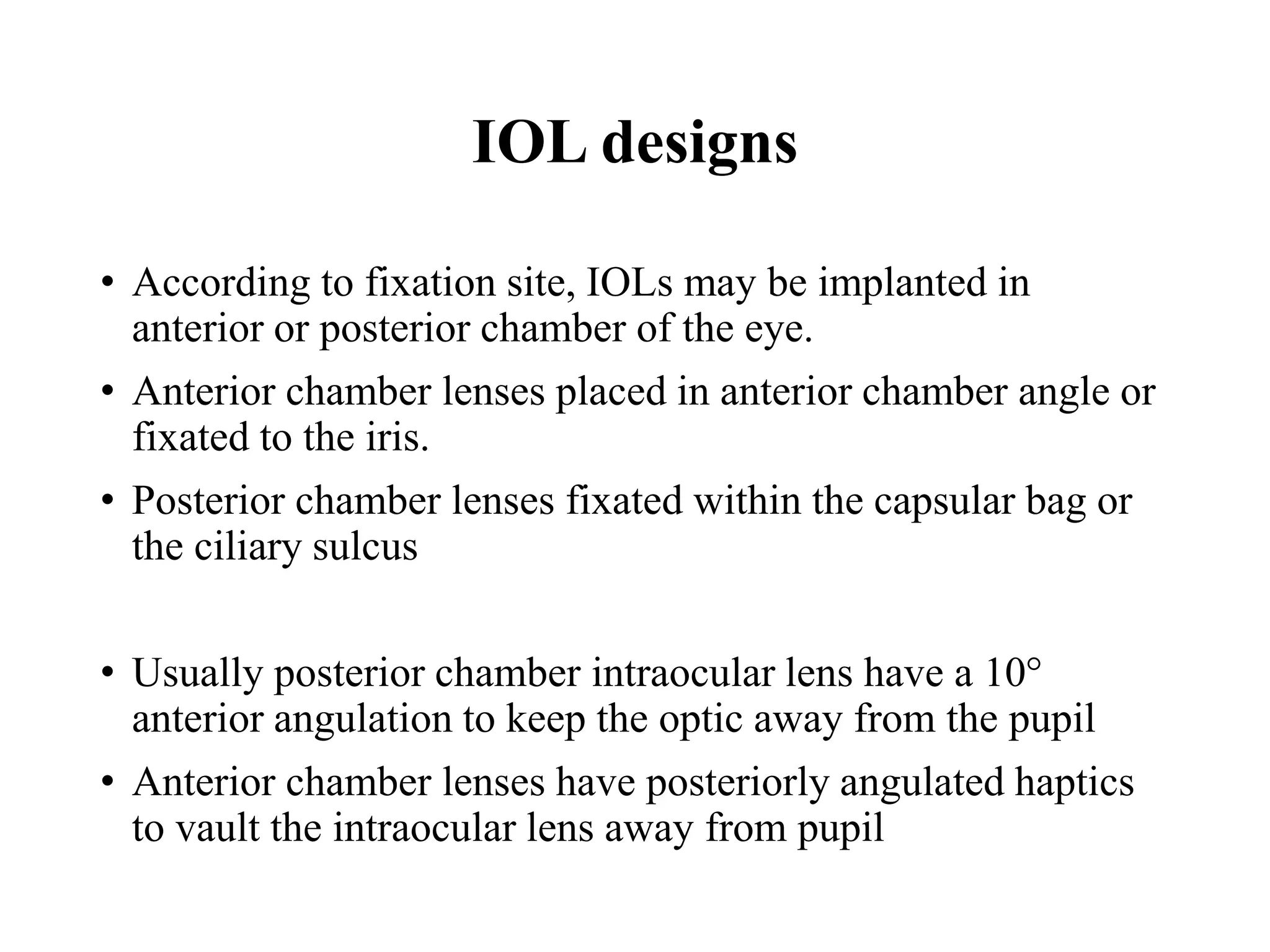
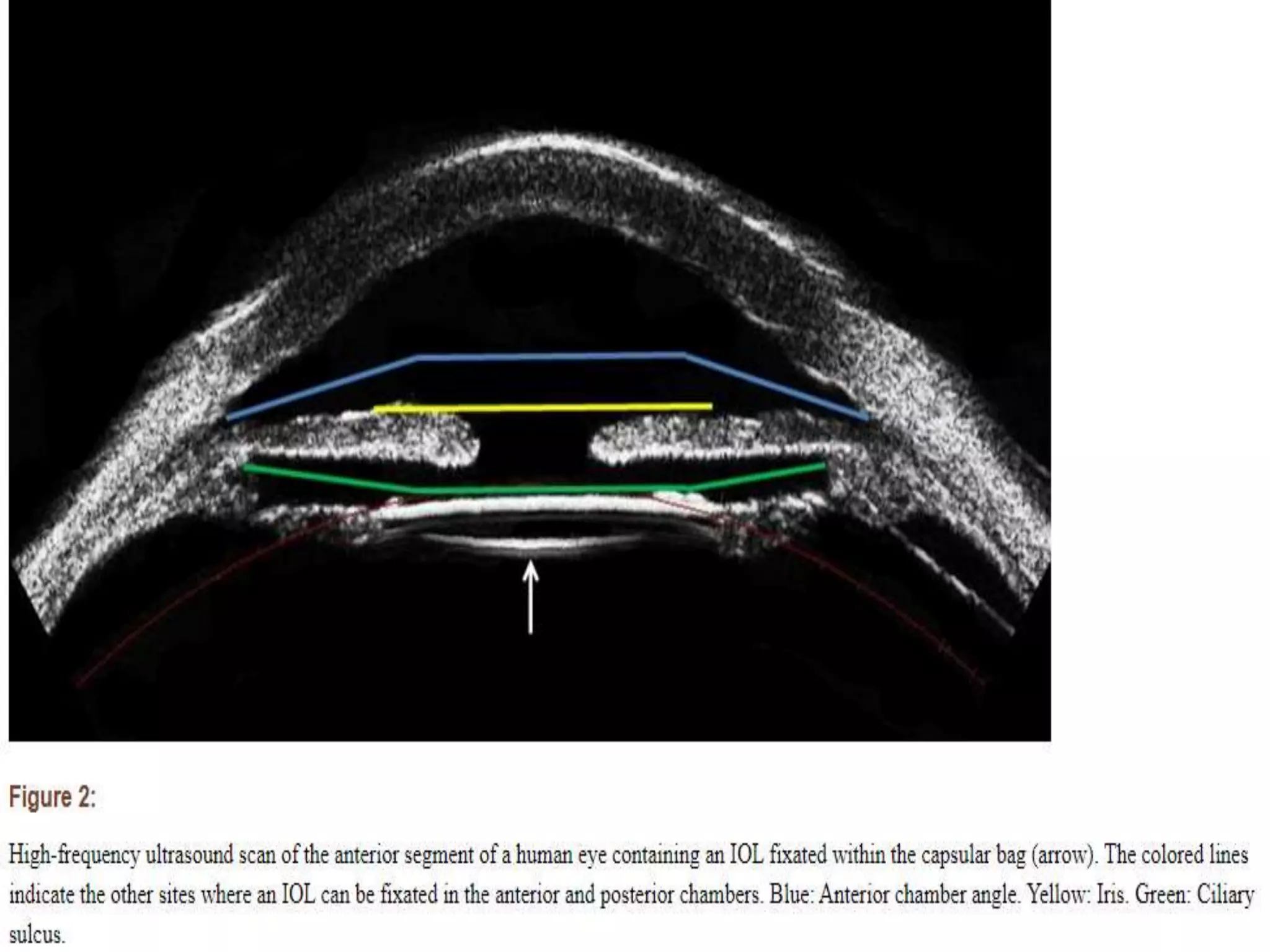
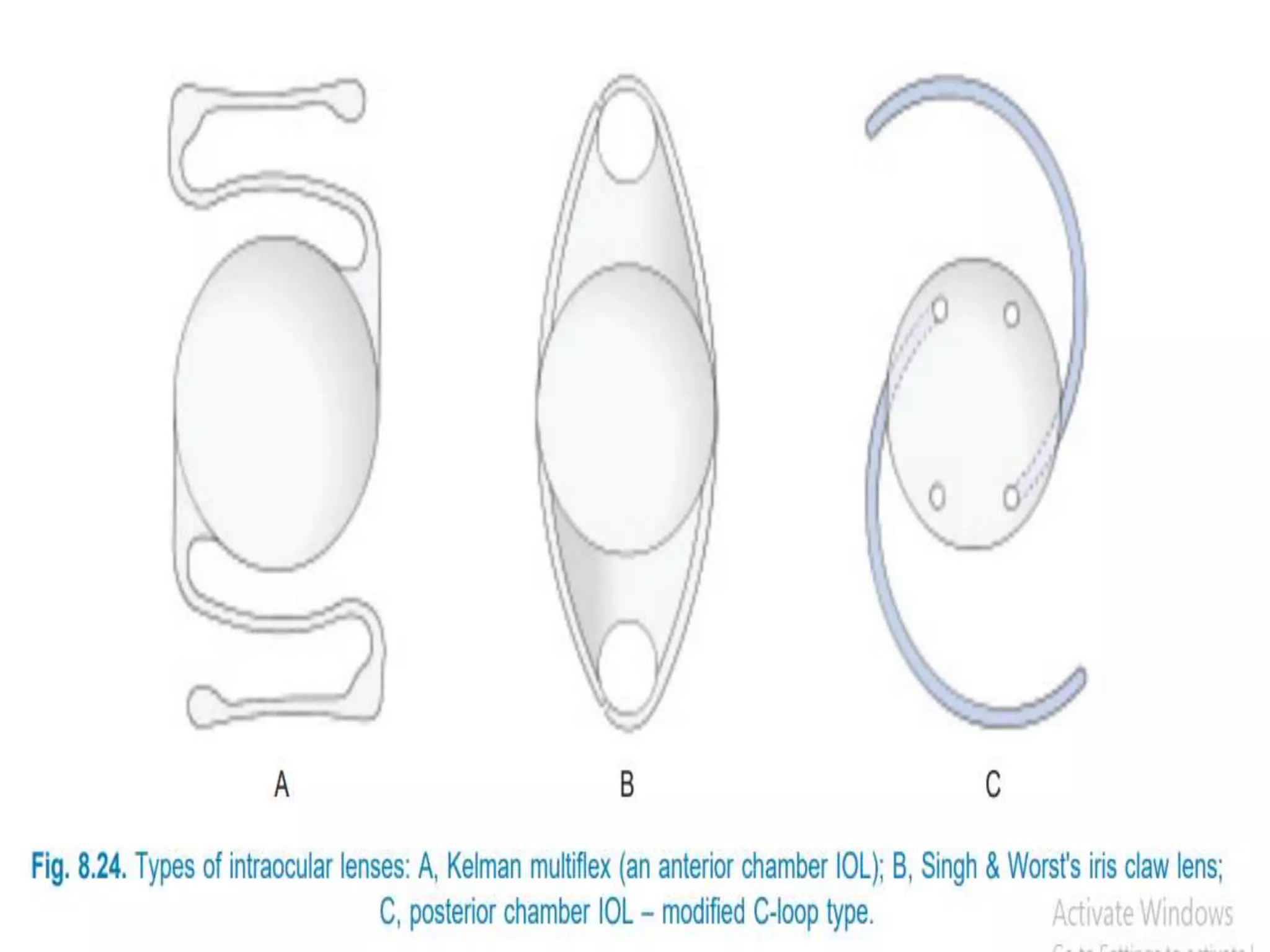
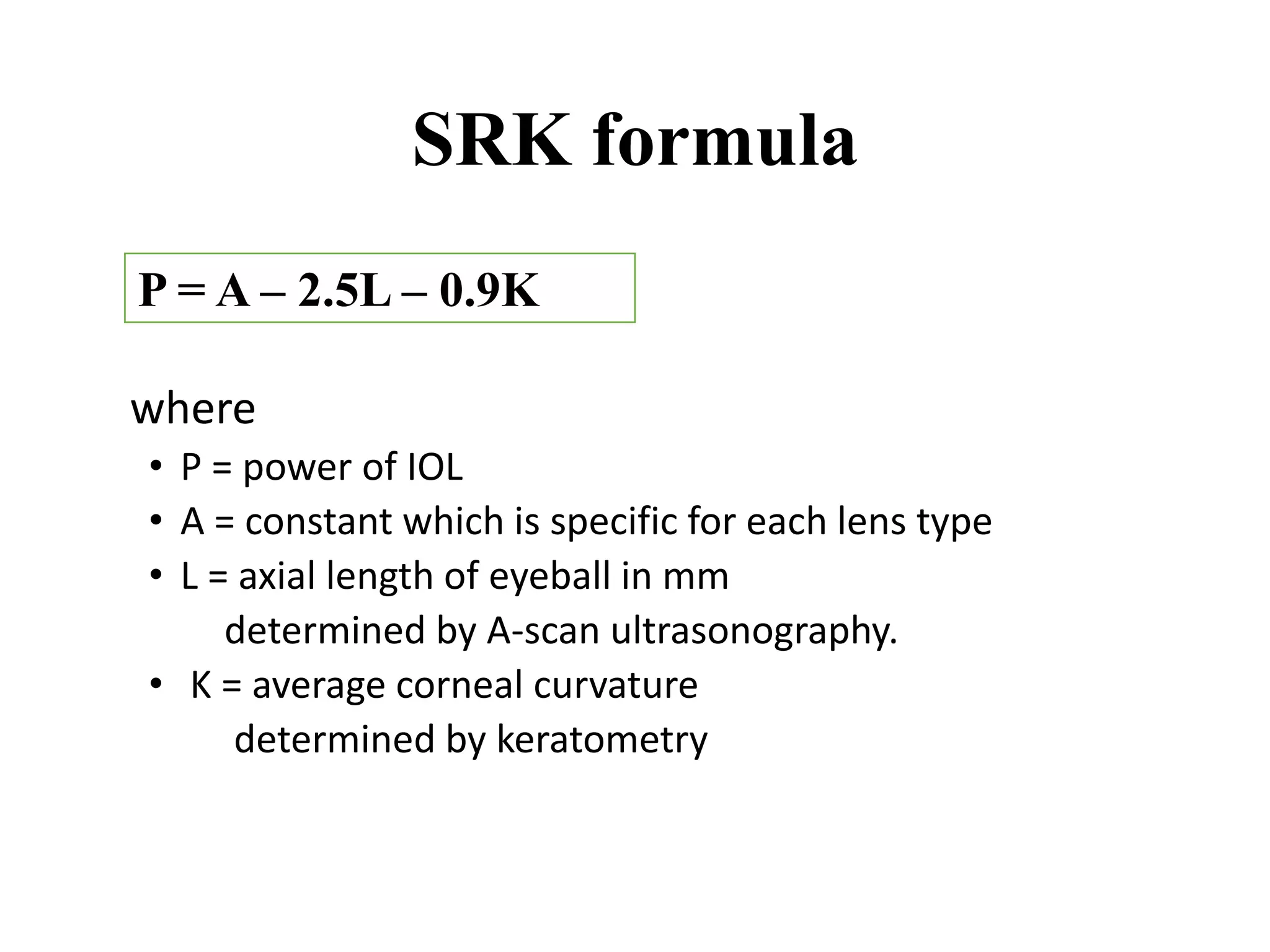

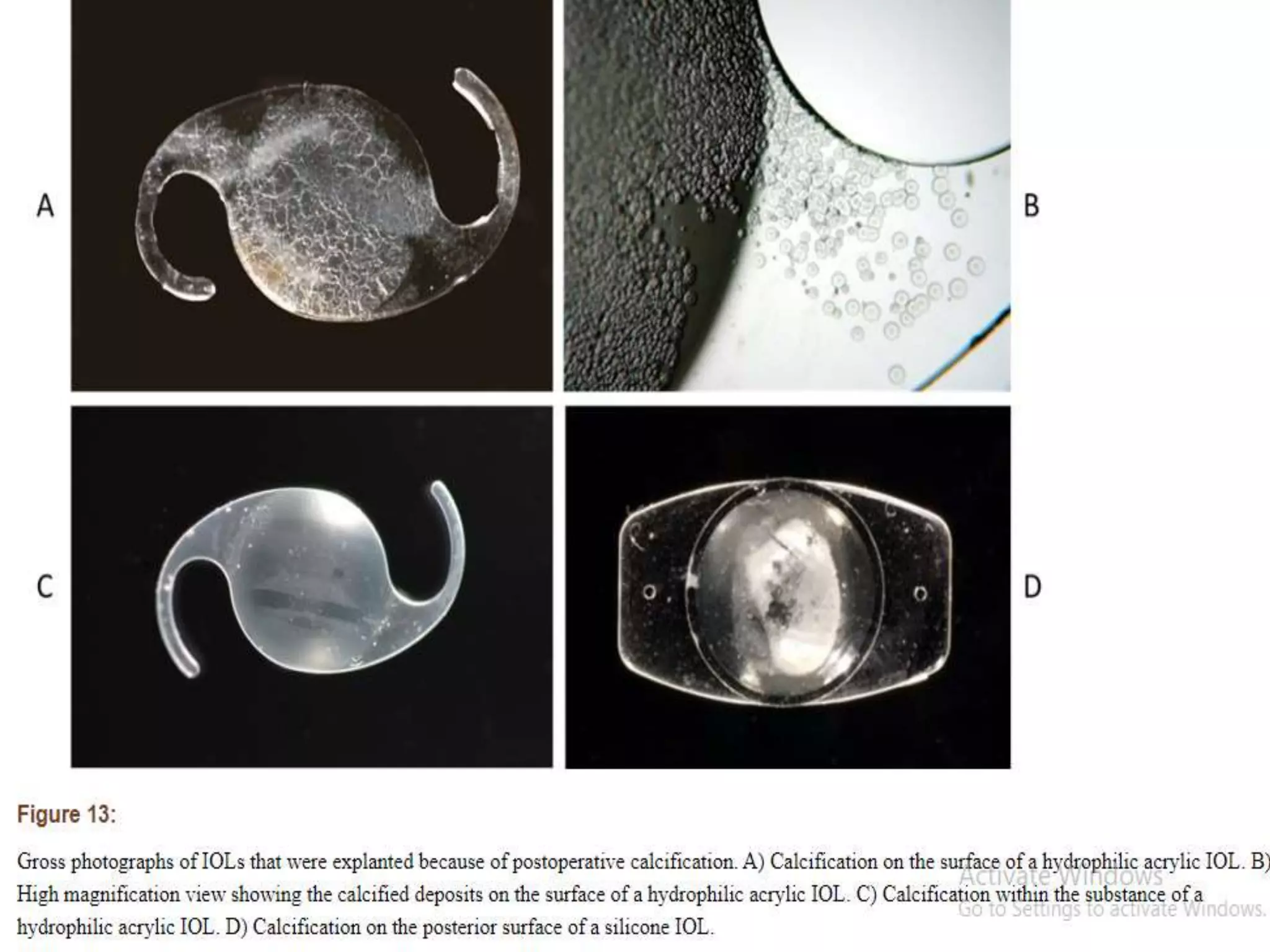
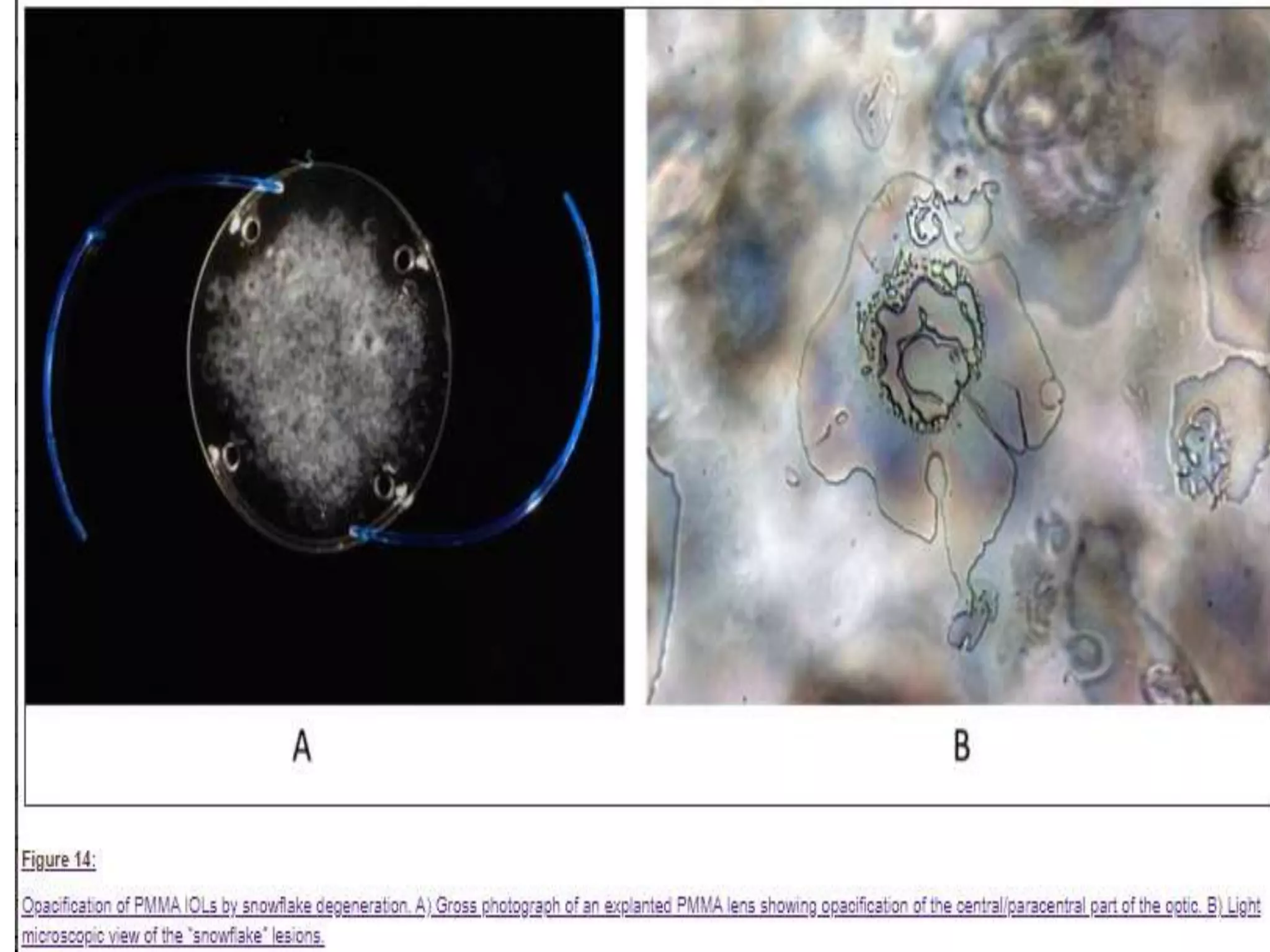
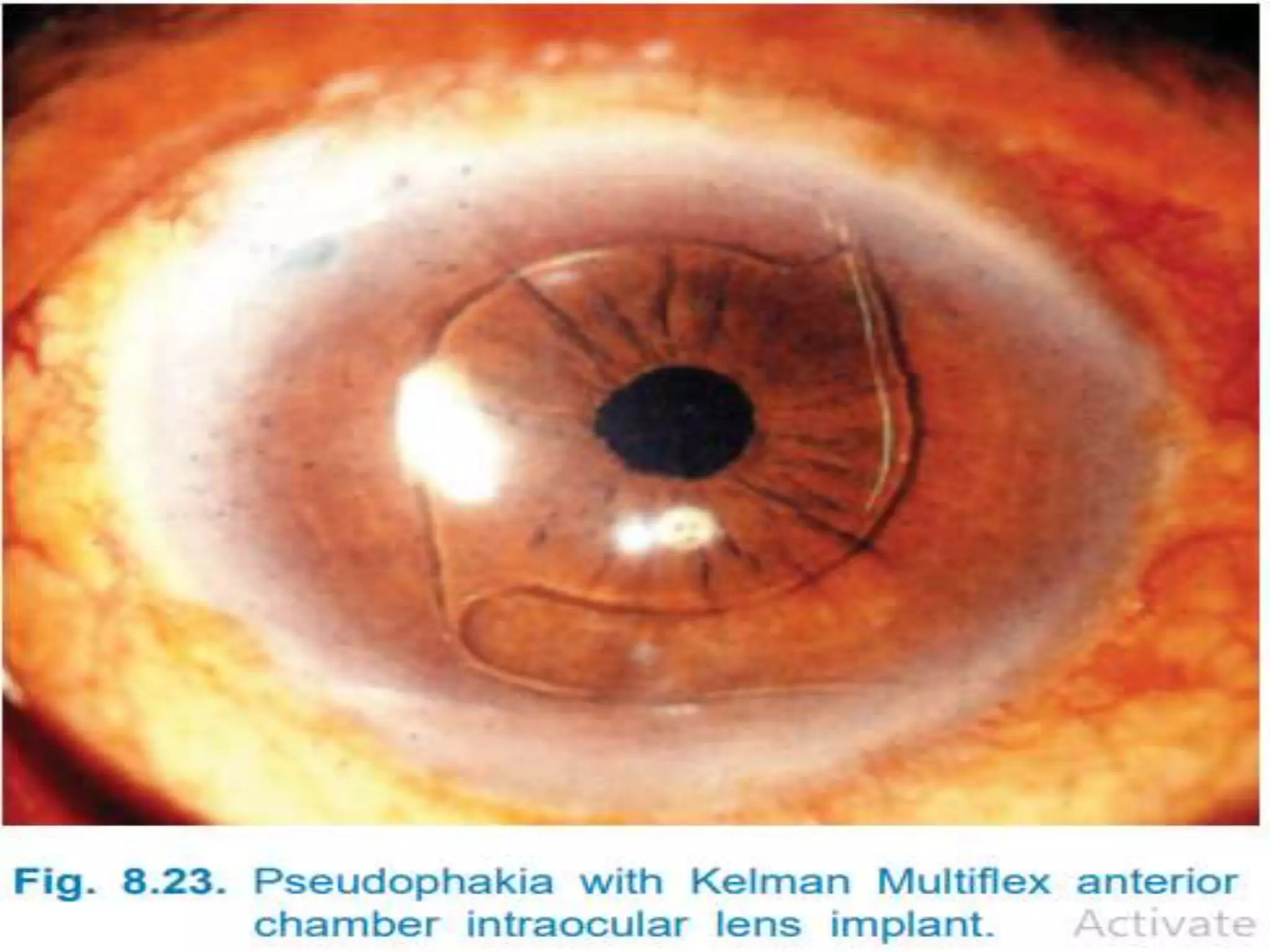

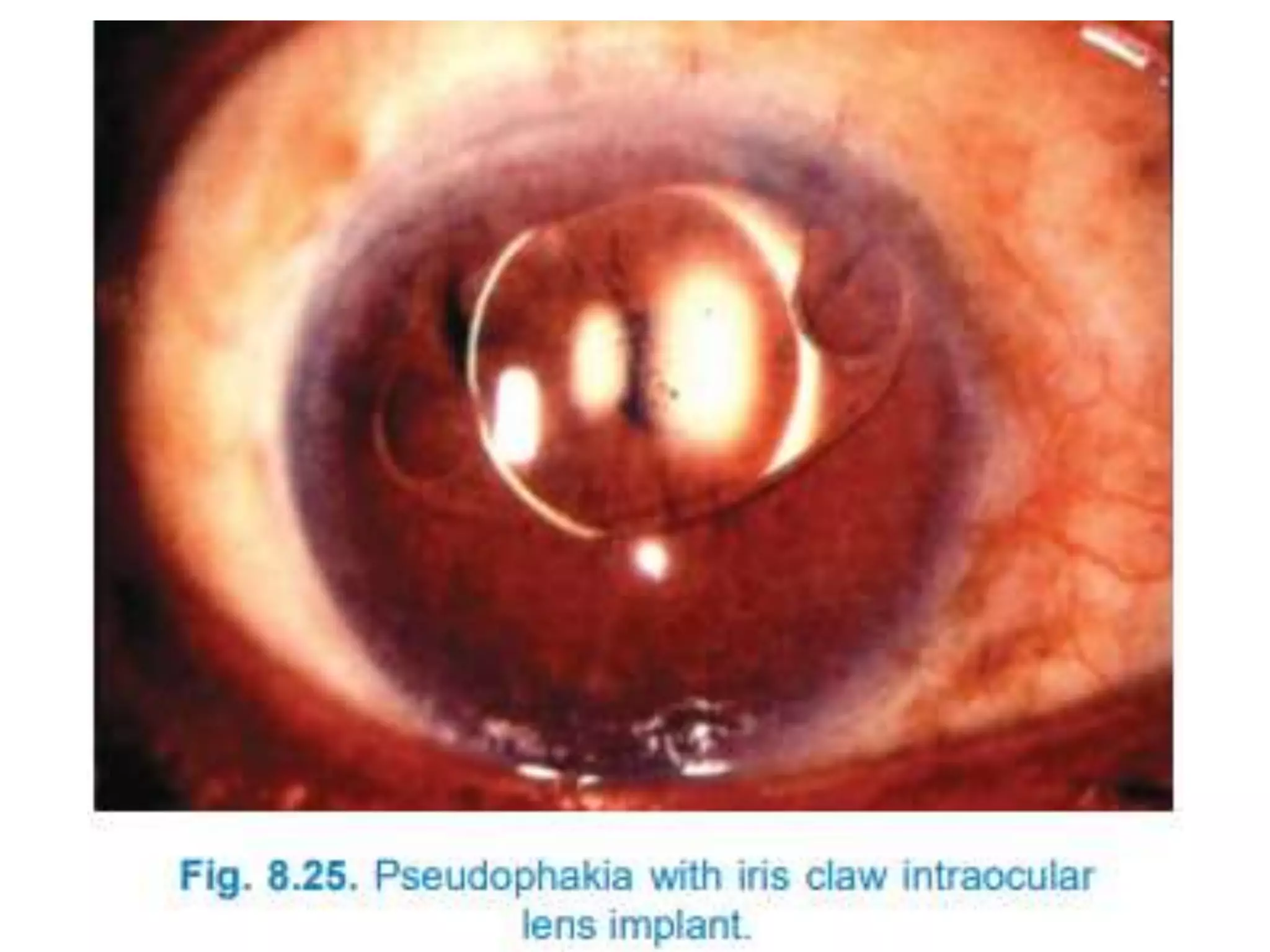



Intraocular lenses (IOLs) are used to restore vision after cataract surgery by replacing the crystalline lens. Sir Harold Ridley first proposed using acrylic plastic lenses for cataracts after observing aircraft plastic fragments in soldiers' eyes did not trigger rejection. IOLs are either single or multi-piece, made of acrylic or silicone, and placed in the anterior or posterior chamber of the eye. Their power is calculated using the SRK formula based on axial length and corneal curvature. Complications can include posterior capsular opacification, calcification, and degradation.





















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
