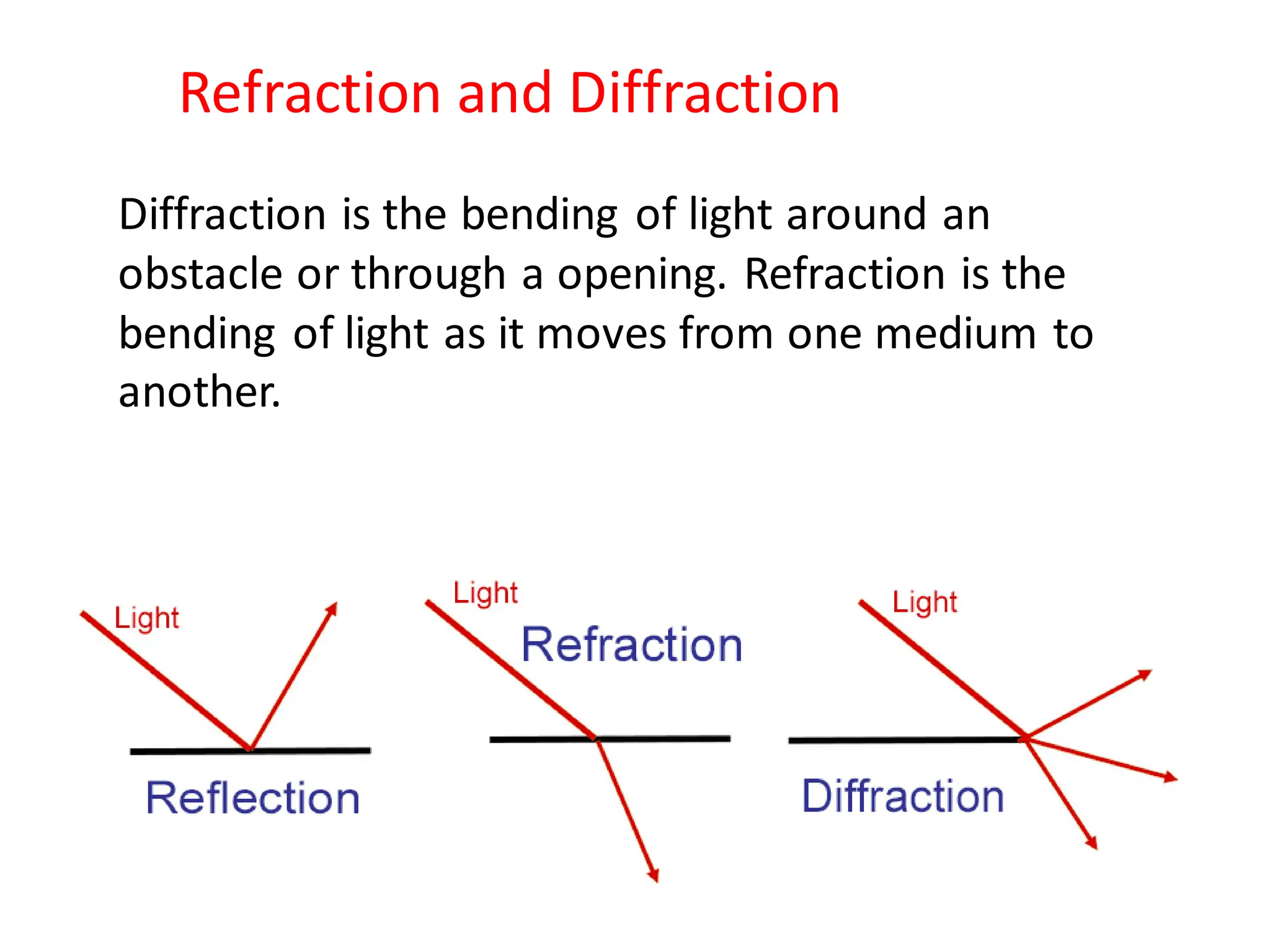
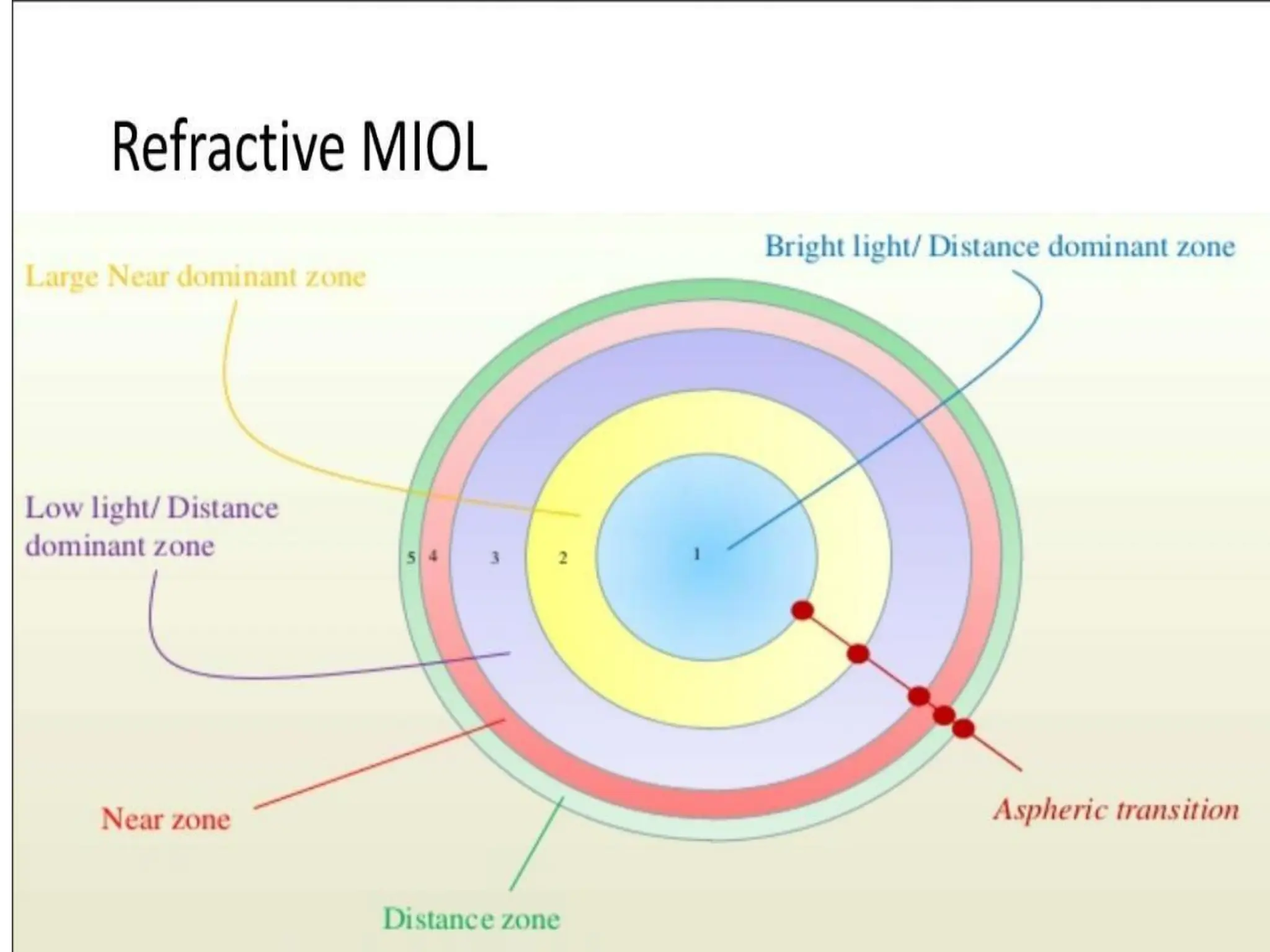
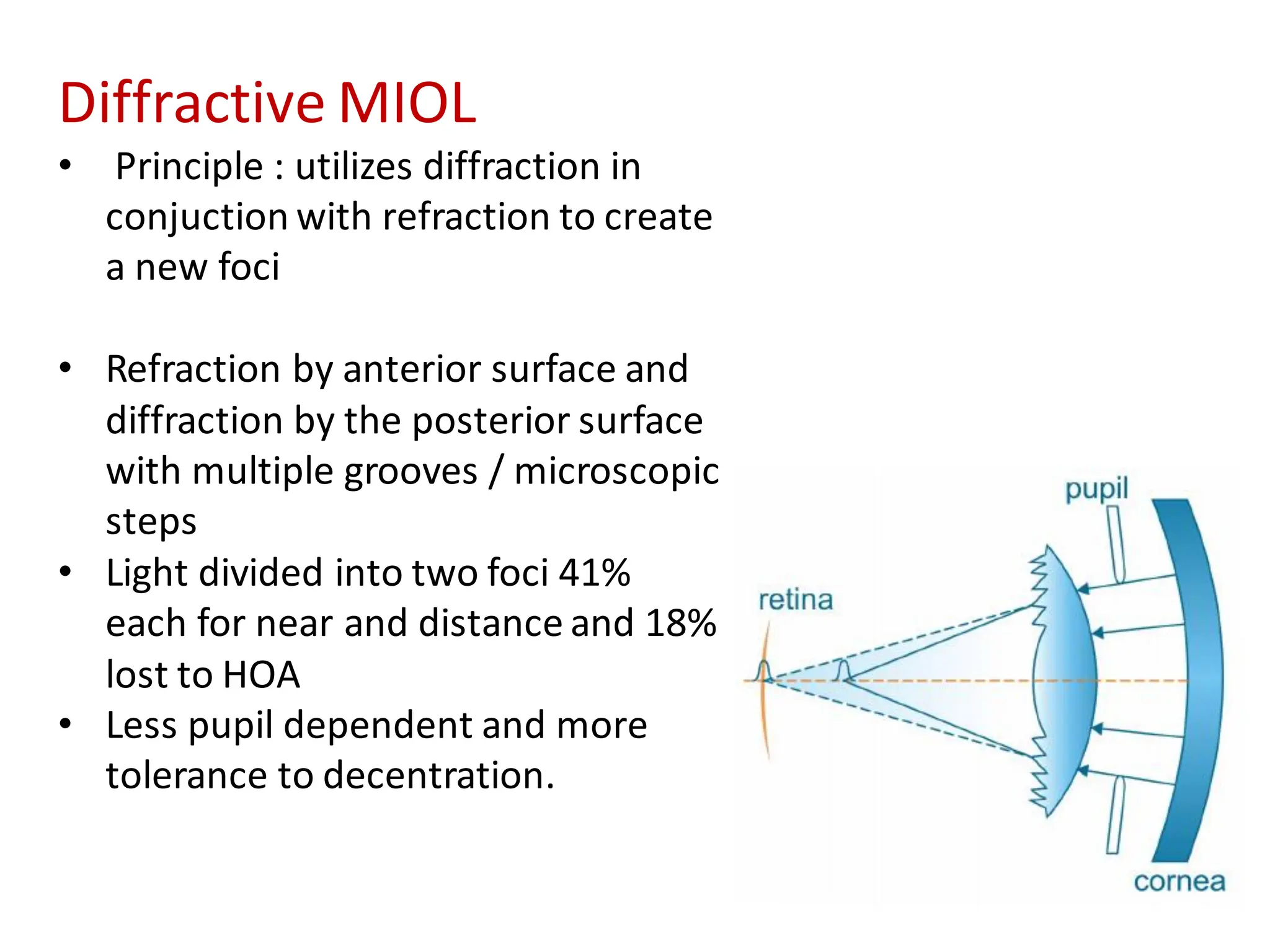
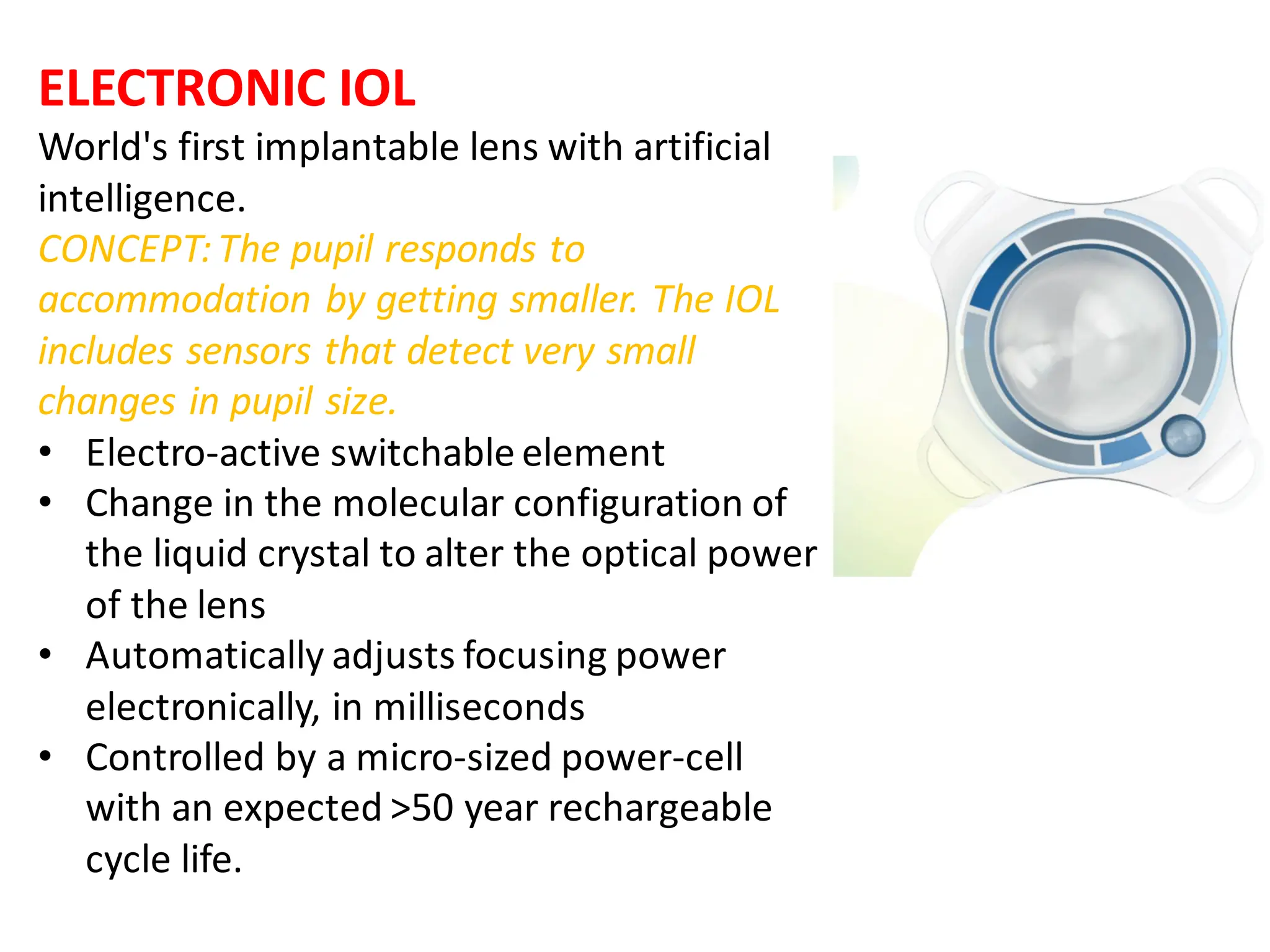
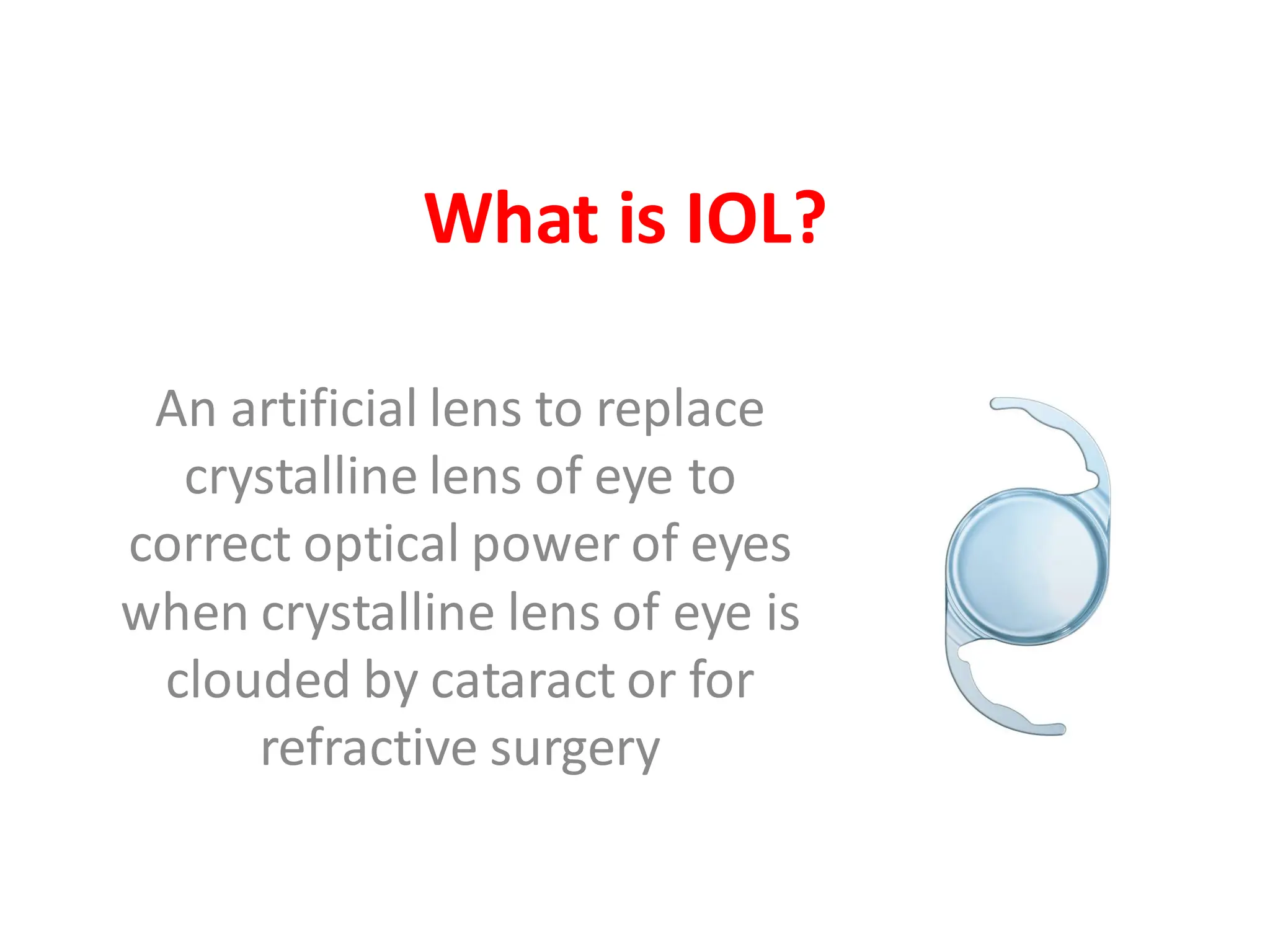
An intraocular lens (IOL) is an artificial lens used to replace the crystalline lens of the eye to correct vision, commonly used for cataract treatment. The document details the history, types, materials, designs, and advancements of IOLs, including multifocal and toric options, as well as their advantages and disadvantages. Over the decades, IOL technology has evolved significantly, improving visual outcomes and accommodating patient needs.
![Collamer
• Patented copolymer of hydrophilic
acrylic and porcine collagen .
• Hydroxyethyl methacrylate
copolymer with a UV absorbing
chromophore.
• Hydrophilic
• In theory, the porcine collagen
improves the biocompatibility of
the lens when implanted in
human eyes.
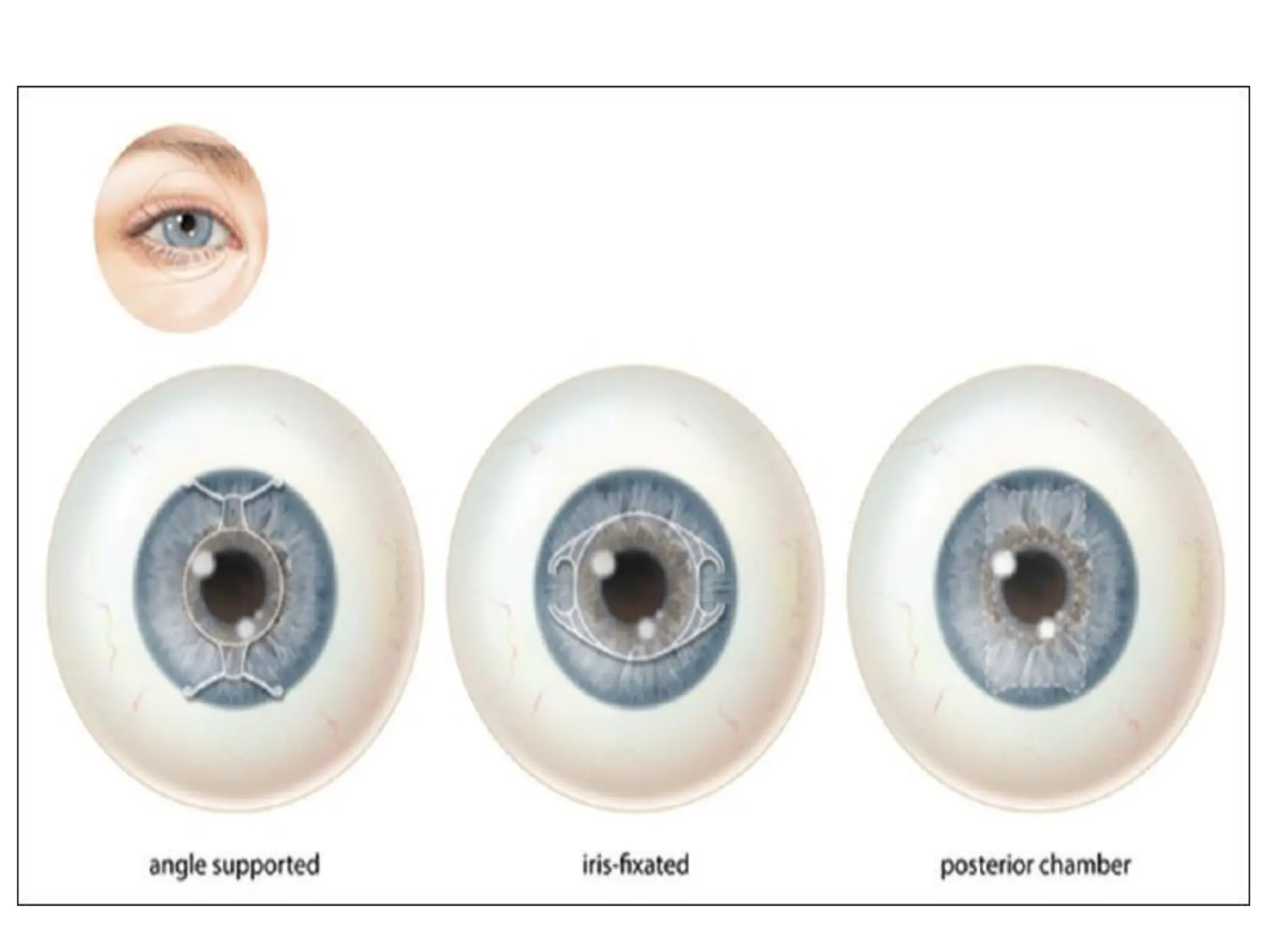
• Mainly used for Posterior
Chamber Phakic Intraocular lenses
[ implantable collamer lens (ICL)]](https://image.slidesharecdn.com/typesofiolandmicrolentics-2-250212173847-f79bc3c3/75/Types-of-IOL-and-Microlentics-2-pdf-iol-p-17-2048.jpg)